Article Text

Abstract
Background Acute coagulopathy of trauma is associated with high mortality and extensive use of blood products. Hemostatic resuscitation, the early administration of blood products with higher ratios of procoagulant components, may improve trauma outcomes in select cases, but can also worsen outcome if inappropriately used. Evolving approaches to hemostatic resuscitation utilize viscoelastic tests to provide a more rational basis for choosing blood component therapy regimens, but these tests are logistically rigorous. We hypothesized that coagulopathy could be detected by the failure of blood clots to remain intact when subjected to a predefined impact force.
Methods We aim to develop a point-of-injury test for coagulopathy. We created coagulopathic blood using an ex vivo normal saline (NS) dilution model and allowed blood of varying dilutions to clot, then examined the behavior of the clotted blood when subjected to a uniform gravitationally induced sheer force.
Results Clots created from coagulopatic blood (diluted to ≤50% with NS) failed under gravitational challenge at a significantly higher rate than non-coagulopathic blood dilutions.
Discussion Impact thromboelastometry (ITEM) represents a simple, logistically lean method for detecting dilutional coagulopathy that may facilitate detection of trauma-induced coagulopathy. ITEM may thus function as a point-of-injury or point-of-care screening test for the presence of coagulopathy.
Level of evidence Diagnostic studies, Level IV.
- Coagulopathy of Trauma
- thrombelastography
- Viscoelastic
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Acute coagulopathy of trauma (ACT) occurs in up to 60% of blunt trauma patients within 30 min of injury, prior to resuscitative hemodilution.1 This state was found to have persisted or worsened by arrival at the trauma center, and occurred in the absence of thrombocytopenia. Similar coagulopathies have also been identified in a variety of other severe illnesses, including sepsis.2
Early identification of ACT allows hemostatic resuscitation, traditionally guided by prothrombin time (PT) testing; most guidelines recognize an international normalized ratio (INR) of >1.5 as indicative of coagulopathy.3 ,4 An INR above this threshold in trauma patients is an indicator of insufficient levels of coagulation factors like fibrinogen, while an INR <1.5 suggests adequate levels of clotting factors.4
Evolving ‘theragnostics’ approaches rely on viscoelastic testing to study clot parameters and direct coagulation factor, platelet concentrate, and antifibrinolytic drug administration.5
INR testing and viscoelastic tests are resource-intensive and sensitive to environmental disturbances, making austere settings (the prehospital arena or at smaller, critical access hospitals) suboptimal for their use.6 ,7
Early detection of ACT could be beneficial: a recent trial of balanced resuscitation showed that high plasma to packed red-cell ratios did not confer survival benefits, possibly because some patients were harmed by unneeded transfusion if not coagulopathic.8 Balanced against this is the recurrent finding of benefit from early administration of clotting factors to patients with ACT, ideally before shock (often with coincident hypothermia) sets in.9
Point-of-injury identification of ACT would foster early, rational treatment, potentially avoiding overtreatment through empiric hemostatic resuscitation protocols. We performed this study to evaluate failure of blood clots formed on a scaffold and subject to a reproducible force as a means of evaluating the viscoelastic strength of clots as a point-of-injury screening test for coagulopathy.
Methods
Study population
We recruited healthy participants aged 18–65 years, who were without illness or injury in the previous week. Participants who were taking medication known to affect coagulation were excluded.
Study design
This was a non-interventional study using a modified activated clotting test. Participants' blood samples were placed in polypropylene tubes containing 6 mg kaolin per mL of blood as a coagulation activator. Tubes contained a full-length copper mesh grid centered within each tube prior to the addition of blood. The grid was made from commercially available copper mesh designed for radiofrequency shielding, cut using a template to 2 mm less than the internal diameter of the sample tubes, with a radius matching that of the tube at the ‘distal’ end. The length of the grid was determined such that the cap held the grid firmly in place, centered in the tube, when the cap was placed. Tubes containing the grid and kaolin were inserted en mass prior to the trial and used in random order.
Samples of whole blood (WB) as well as blood diluted with normal saline (NS) to 75%, 50%, 40%, and 30% blood were utilized. Prefilled NS flush syringes premeasured to the specific sample dilution were used to draw blood via a cannula extension. The INR of selected samples (50% and 30% blood) was determined using an iStat Point-of-care device and recorded.
Study procedures
Participants provided informed consent, then underwent an assessment consisting of measurement of vital signs and a medical interview to ascertain the presence of any exclusion criteria.
An intravenous cannula was then inserted in each participant's accessory cephalic vein to facilitate sample blood collection. We used syringes prefilled with NS flush and drew the indicated volume of blood into each, then inverted tubes four times to mix.
Samples (5 mL volume) were transferred to tubes containing the clot activator and copper mesh as described above. Tubes were prelabeled with a unique identifier assigned to each participant along with the dilution schedule contained in that particular tube.
Tubes were then inverted to facilitate kaolin dispersion. Two tubes at each dilution were prepared. Immediately after mixing, tubes were placed upright (in random order) between the participant's thighs for incubation for 15 min.
During the incubation period, INR testing was performed utilizing a precalibrated iSTAT device and the results were recorded for the chosen dilutions.
If no visible clot formed during incubation, this was be taken as evidence of severe coagulopathy, as was failure of clot adherence to the grid on tube inversion. Tubes in which clot remained adherent were subjected to a ‘drop test’ that is, inverted and dropped cap-down on to the floor through a 75 cm PVC pipe (held perpendicular to the floor adjacent to participants). The pipe served to keep the tube vertically oriented and standardize the drop height. The operator examined the sample tube and results were recorded (whether the clot was intact vs failed, as well as the dilution indicated).
Statistical analysis
Statistical analysis utilizing paired tests compared proportions of failed clots at each dilution of blood with undiluted blood. The average INR for each selected dilution was also determined. Stata V.14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, Texas: StataCorp LP) was used for statistical calculations.
Results
We recruited 12 participants, ageing from 21 to 45; 4 were women. None reported the use of anticoagulant or antiplatelet medications, and all denied having sought care within the previous week for illness or injury. Females denied pregnancy. All patients had normal HR, BP, and SaO2, and were normothermic.
Intravenous access was established on the first attempt in all participants. Two had complications related to venipuncture: one had a self-limited vagal response, and one developed petechiae from the venipuncture tourniquet. Both participants improved spontaneously and were later asymptomatic.
A total of 119 ‘drops’ were completed, with one sample lost due to lid failure on inversion. Figure 1 shows examples of intact and failed clots. Discordant results between drop 1 and drop 2 occurred in 12 sample pairs.

Examples of failed (two tubes, left) and intact (two tubes, right) clots after impact thromboelastometry.
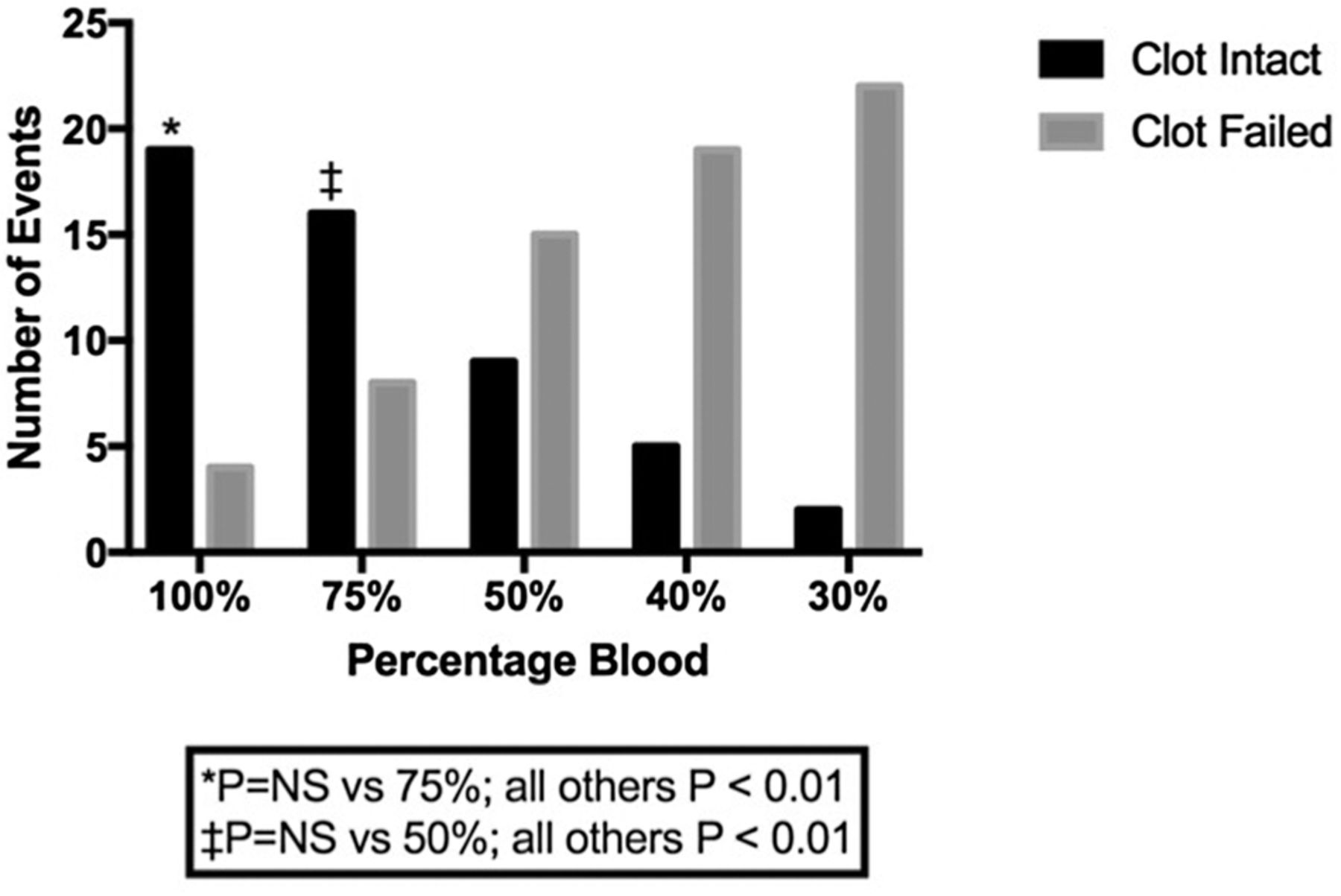
Clots from WB and 75% blood failed in 17.3% and 33.3% of drops, respectively, while clots from 50%, 40%, and 30% blood failed 62.5%, 79.1%, and 3.8% of drops. Differences between WB and 30–50% blood were significant to p<0.01, as were differences between 75% blood and 30–40% blood. Table 1 lists clot behavior for each sample concentration of blood. Figure 2 shows failed versus intact clot stratified by percentage of blood in samples subjected to drop testing.
Drop test results by percentage blood
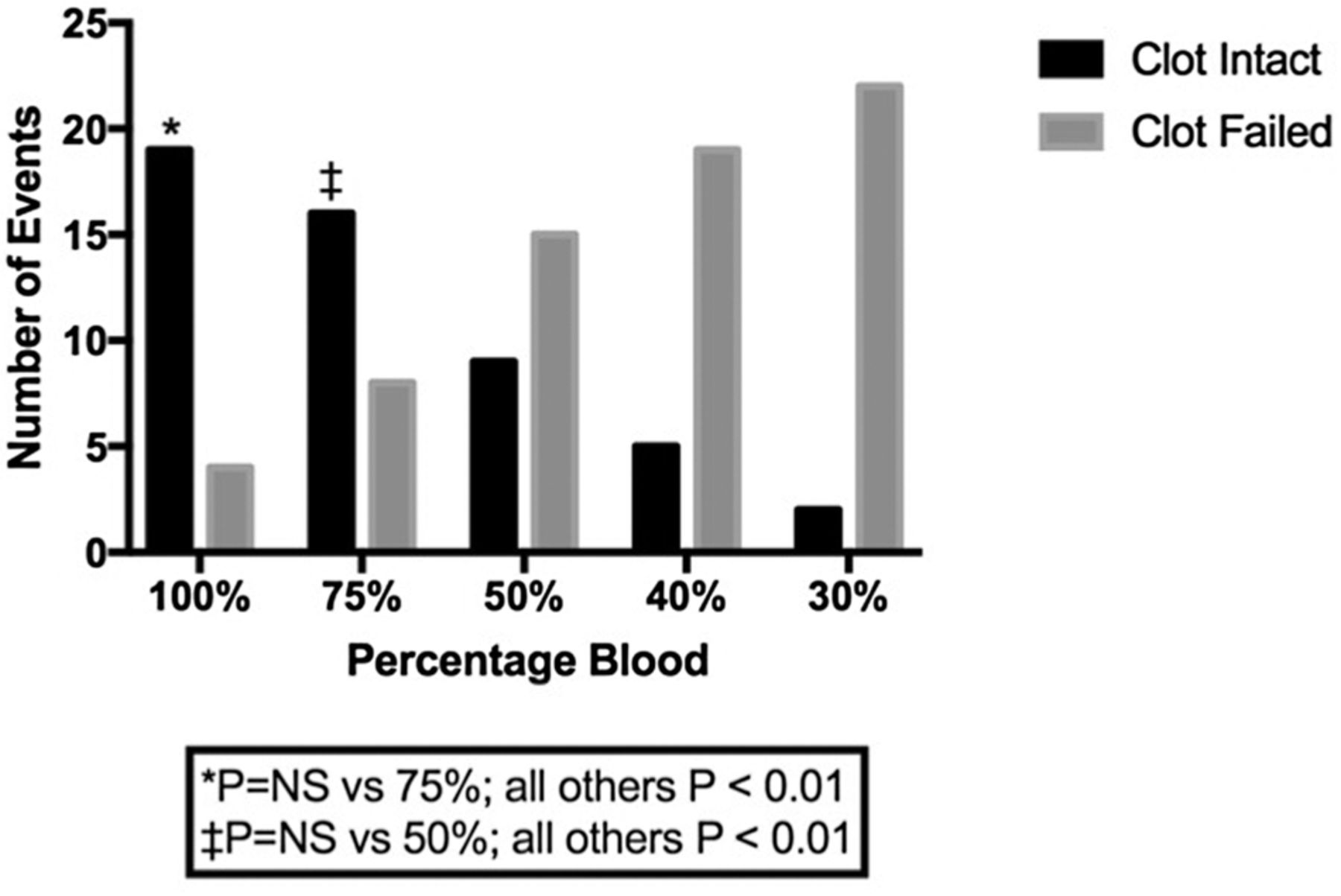
Results of impact thromboelastometry test by sample composition (%blood).
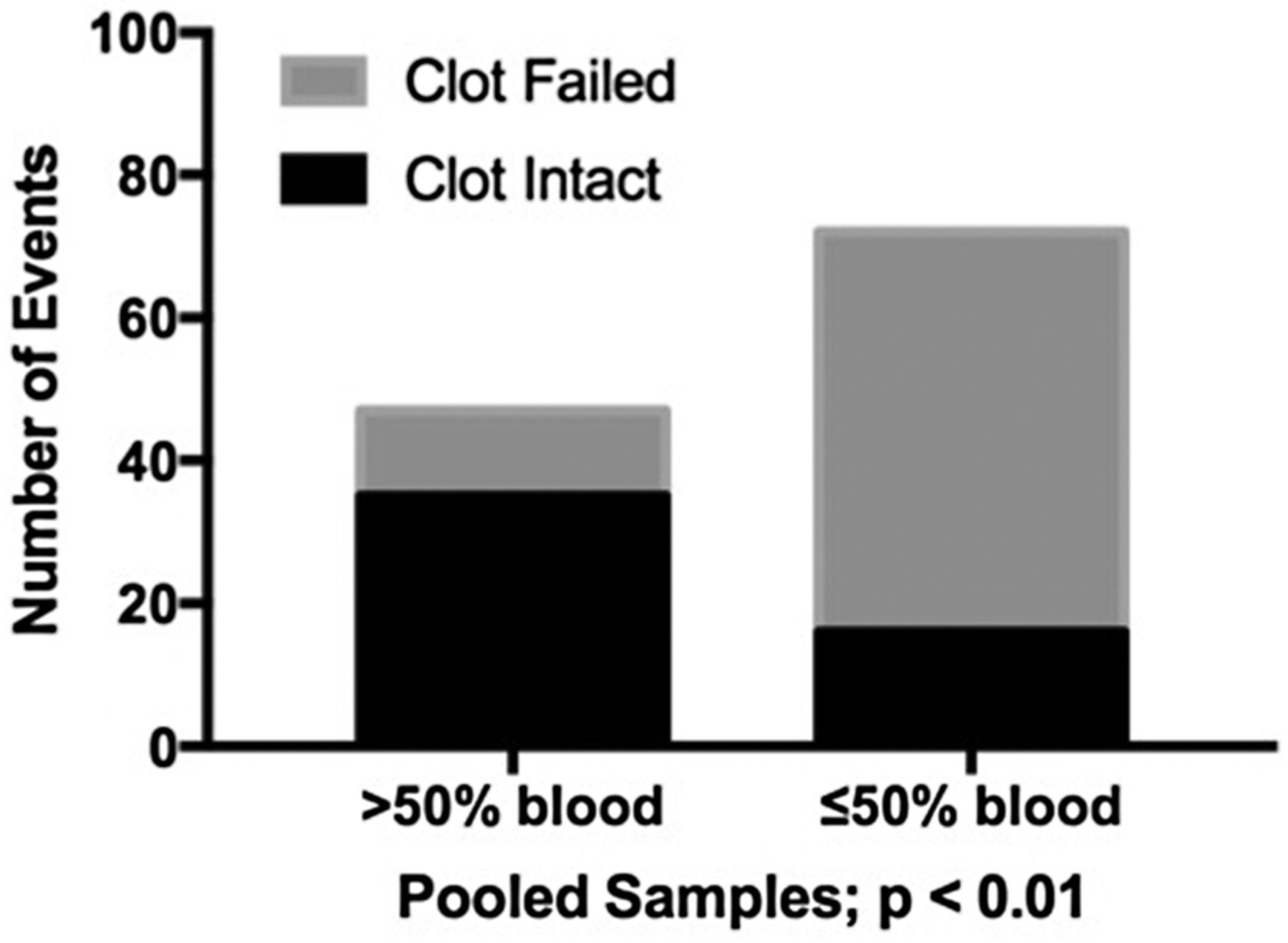
Figure 3 compares grouped results for samples unlikely to be coagulopathic (75–100% blood) with samples likely to be coagulopathic (prior work showed that blood diluted to <60% is coagulopathic10). The average INR for blood diluted to 50% was 1.58±0.28; the average INR for blood diluted to 30% was 4.9±1.66.
{kind=link}
{kind=link}
{kind=link}
Pooled results of impact thromboelastometry for non-coagulopathic (75–100% blood) and coagulopathic ≤50% blood) samples.
Discussion
Multiple modalities exist for the detection of ACT. International health providers use ‘whole blood clotting’ tests (WBCTs) to identify coagulopathy (due largely to hypofibrinogenemia) in snakebite victims, surgery patients, and others.11 WBCTs lack objectivity for the purpose of guiding blood component therapy.
The activated clotting time is a measure of the common pathway of coagulation. Mattox and colleagues showed that prolonged intraoperative activated clotting time was associated with surgeon perception of need for damage control surgery protocols and massive transfusion. They described activated clotting time as ‘a sensitive, rapid and inexpensive indicator of the global coagulation status in operative trauma victims’.12
Given that the activated clotting time is a WB test, the effects of platelets on clot and the effects of trauma and resuscitation on the cellular components are likely to be more visible with activated clotting time than with serum-based PT/INR. On the other hand, the activated clotting time does not specifically detect changes in clot strength or stability.13
Widely employed coagulation tests such as PT/INR and partial thromboplastin time were developed to monitor medication effects on clotting initiation, and do not evaluate cellular components. Viscoelastic tests like TEG (Haemonetics Corporation, Braintree, Massachusetts, USA) and ROTEM (Tem International GmbH, Basel, Switzerland) are used in an expanding range of clinical scenarios to assess coagulation status in acutely ill medical and surgical patients. TEG and ROTEM offer the advantages of being performed on WB, allowing assessment of clot parameters (speed, strength, and stability); adequacy of these is essential for hemostasis and fosters the preservation of intravascular volume and oxygen-carrying capacity.
Objective point-of-injury identification of coagulopathy in critically ill patients may allow expeditious intervention using fresh-frozen plasma and with newer agents like prothrombin complex and fibrinogen concentrates. Empiric treatment with these agents, conversely, can worsen morbidity in patients absent coagulopathy.8 ,14–17 Clearly, the gap between diagnosis of ACT and its treatment calls for a simple, objective, reliable, and widely deployable bridge.
Viscoelastic tests utilize sheer and strain measurements to evaluate clot parameters, prompting the lead author to ask if other mechanisms of inducing sheer could offer useful information about clot parameters in austere circumstances. The goal of hemostatic resuscitation is fast formation of strong, stable clots; impact thromboelastometry (ITEM) may allow detection of differences in coagulation jeopardizing this combination of traits. We developed ITEM as a point-of-injury adjunct to current viscoelastic tests. ROTEM and TEG have logistical requirements that limit their use to advanced facilities such as designated trauma centers, solid-organ transplant centers or hospitals performing cardiac bypass.
Prior work using TEG in an ex vivo model showed that hemodilution in excess of 50% with NS impairs clot initiation (R), clotting speed (α), and clot strength (MA).10 While other factors such as red blood cells, platelets, and other clotting factors are diluted in these models, prior investigations by Martini18 using animal models have suggested that hypofibrinogenemia is the major change leading to deficits in the speed, strength, and stability of clots.
Using a similar hemodilution model, we demonstrated that thromboelastometry utilizing sheer force induced by a drop of 75 cm to a hard surface causes clotted blood previously hemodiluted with NS to ≤50% to fail in the majority of trials, while clots from lesser dilutions tend to remain intact. We infer that significant coagulopathy was induced in our higher dilutions of blood based on our finding that the average INR for 50% blood is 1.6 (vs <1.5 as the traditional definition of coagulopathic4).
Clot failure may indicate impairment of either platelet or clotting protein function or both. Incubation by keeping the tube between skin surfaces is potentially more physiologically meaningful than routine laboratory-based 37° incubation in cases where hypothermia has supervened, such as in some prehospital scenarios. Many ROTEM studies match machine to patient temperature,19 so our ‘patient incubator’ represents a point-of-injury equivalent, allowing examination of the effect of the patient's body temperature on hemostasis.
This study should be interpreted within the context of several limitations. First, this was a feasibility study, and it served its purpose. Our study was preliminary and has the limitations inherent to an ex vivo test. Given budgetary restrictions, we were not able perform INR testing on all samples, nor to apply gold-standard viscoelastic tests to complete evaluation of hemostasis in this investigator-funded study. Despite these limitations, ITEM is conceptually sound and technically feasible: on exposure to a standardized force of impact-induced sheer, clots of coagulopathic blood fail to stay intact; there is a strong trend toward failure of clots under ITEM with higher dilutions. ITEM holds significant potential for the care of patients sustaining injury by simplifying the assessment of coagulopathy, extending detection of coagulopathy into austere settings via an inexpensive, logistically lean test which may also have utility in other scenarios where coagulopathy complicates care such as sepsis and severe maternal hemorrhage.20
Before this technique can be adopted, studies using comparison viscoelastic tests, platelet counts and fibrinogen levels are indicated. Additionally, the specific coagulation component deficits (of fibrinogen vs platelets, eg) identifiable by ITEM and the ideal parameters for use of this technique need to be defined.
Conclusion
ITEM is a point-of-injury screening test for coagulopathy with advantages for field use: lightweight, compact design; tolerance of forces delivered during transport and storage; and ease of use without need for power, water, or gas supplies. ITEM requires little training to operate and is not logistically onerous while being robust and physiologically relevant.
References
Footnotes
Contributors GSD designed the study. GSD, AAT, and JNH collected and processed data and managed the study and databases. GSD, AAT, and JNH prepared and edited the manuscript.
Competing interests None declared.
Ethics approval University of Utah IRB.
Provenance and peer review Not commissioned; externally peer reviewed.