- 1Department of Surgery, Creighton University School of Medicine, Omaha, Nebraska, USA
- 2Division of Trauma Surgery and Surgical Critical Care, Creighton University Medical Center, Omaha, Nebraska, USA
- Correspondence to J A Asensio; juanasensio{at}creighton.edu
- Received 12 July 2016
- Revised 1 August 2016
- Accepted 2 August 2016
- cardiac arrest
- traumatic hemorrhage
- penetrating cardiac or great vessel injury
A 28-year-old man sustained multiple stab wounds. During transport by emergency medical services, the patient suffered cardiac arrest and required cardiopulmonary resuscitation (CPR).
On arrival, he was ‘in extremis’. Vital signs: blood pressure 58/33 mm Hg; pulse 144 bpm; respiratory rate 33 bmp; and oxygen saturation 85%. He was immediately intubated. In the right femoral and subclavian veins 8.5 French catheters were placed. Fluid resuscitation was started using Lactated Ringer's, 2 units of uncross-matched packed red blood cells (PRBCs) and 2 units of fresh frozen plasma (FFP).
Physical examination revealed 6 non-bleeding stab wounds, 2–3 cm each, located 1 cm below the right midclavicular line; 1 cm lateral and below the left sternoclavicular junction; 1 cm below and 2 cm medial to the right scapula; 2 cm medial to the midborder of the left scapula; in the right abdominal flank, at the posterior axillary line, 3 cm above the right iliac crest; and a right anterior midthigh wound.
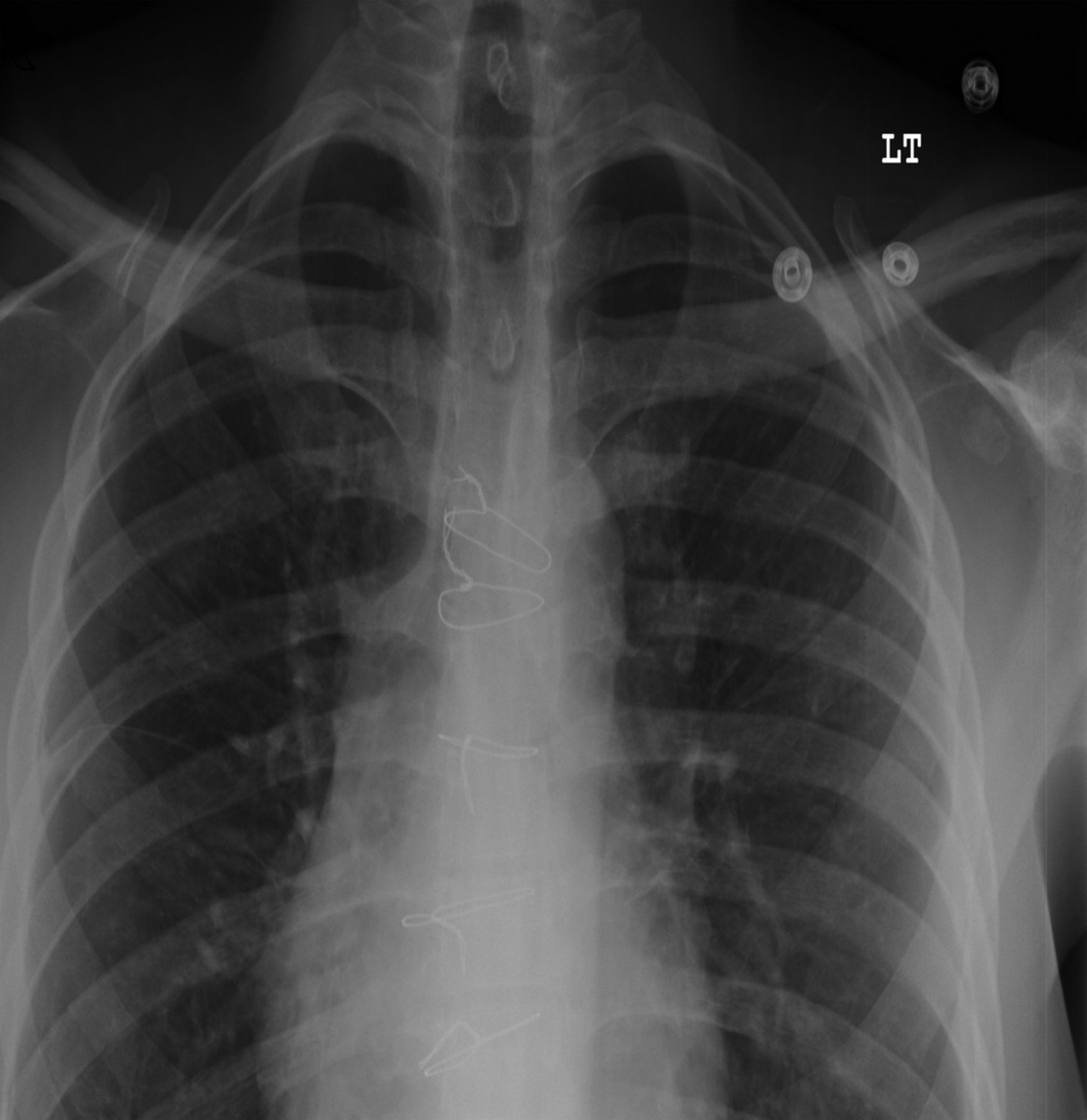
The patient had decreased breath sounds in both hemithoracic cavities. Bilateral 36 French chest tubes were placed at the fifth intercostal spaces. The right-sided chest tube produced 500 mL of blood, the left produced 1 L. A focused assessment with sonography for trauma (FAST) scan revealed significant fluid in the pericardium. A chest X-ray (figure 1) revealed moderate hemothorax on the right and large hemothorax on the left.

A chest X-ray revealing proper placement of chest tubes with a moderate amount of retained hemothorax on the right and a large retained hemothorax on the left.
Another 2 units of uncross-matched PRBCs were administered; massive transfusion protocol was activated. The patient remained hypotensive with pressures between 60s and 80s and his heart rate decreased from 140s to 120s. Arterial blood gas readings were pH 7.12/PaCO2 48/PaO2 66/HCO3 15.6/O2 saturation 84%/lactic acid level 20.4.
What would you do?
Left anterolateral thoracotomy;
Simultaneous median sternotomy and laparotomy;
Median sternotomy;
Bilateral anterolateral thoracotomies;
Left anterolateral thoracotomy and simultaneous laparotomy.
What we did and why
Correct answer: C
The patient was rapidly transported to the operating room (OR) where we performed median sternotomy as the best approach; since he had a pericardial tamponade clinically and by FAST as well as a suspected left subclavian injury. Had we selected a left anterolateral thoracotomy, this would have allowed us access to the heart and left lung; however, it would have had to be converted to a median sternotomy along with a left infraclavicular incision for exposure of the left subclavian artery. Bilateral anterolateral thoracotomies are a reasonable approach for cardiac and bilateral pulmonary injuries but would have posed challenges for the exposure of a potential left subclavian arterial injury and in this case, a left internal mammary injury. Laparotomy was not warranted as wound exploration in the OR revealed no peritoneal violation.
Within the pericardium, a large quantity of blood and thrombus were evacuated; no injuries were noted to cardiac chambers. Hemorrhage was noted below the left sternoclavicular junction. The left pleuropericardial reflection was incised, revealing a transection of the left internal mammary artery ∼1 cm below its origin from the left subclavian artery. This was doubly ligated with a 2-0 silk suture. The patient remained profoundly hypotensive and experienced his first intraoperative cardiopulmonary arrest. He required CPR, epinephrine, and defibrillation with 20 J; this restored the cardiac rhythm.
In the left hemithorax, a larger retained hemothorax was evacuated. The pulmonary hilum was digitally occluded simultaneously, while a central stapled pulmonary tractotomy with selective deep vessel ligation was performed. This revealed a lacerated lingular artery that was sutured. Argon beam coagulator was used to control bleeding and oozing from the transected pulmonary parenchyma. A second cardiopulmonary arrest ensued, and the patient was successfully resuscitated. The right pleuropericardial space was accessed and a 3 cm actively bleeding laceration was found in the right upper lobe. A stapled pulmonary tractotomy with selective deep blood vessel ligation was performed.
The patient subsequently experienced a third cardiopulmonary arrest. He developed a large dilated right atrium and ventricle, indicative of right ventricular failure; along with a non-pumping left ventricle. Right ventricle was unloaded by venting with a 14-gauge angiocatheter, 200 mL of blood were removed, 12.5 g of mannitol and 5 mg of furosemide were administered. These maneuvers, CPR and defibrillation restored a normal cardiac rhythm.
Physiological derangements, caused by the lethal tetrad of acidosis, hypothermia, coagulopathy, and dysrhythmias began to reverse. Pulmonary parenchyma was approximated. A 32 French curved chest tube was placed below the right xiphisternal junction, directly into the pericardial recess and a 36 French straight chest tube was placed below the left xiphisternal junction. Pleural cavities were drained.
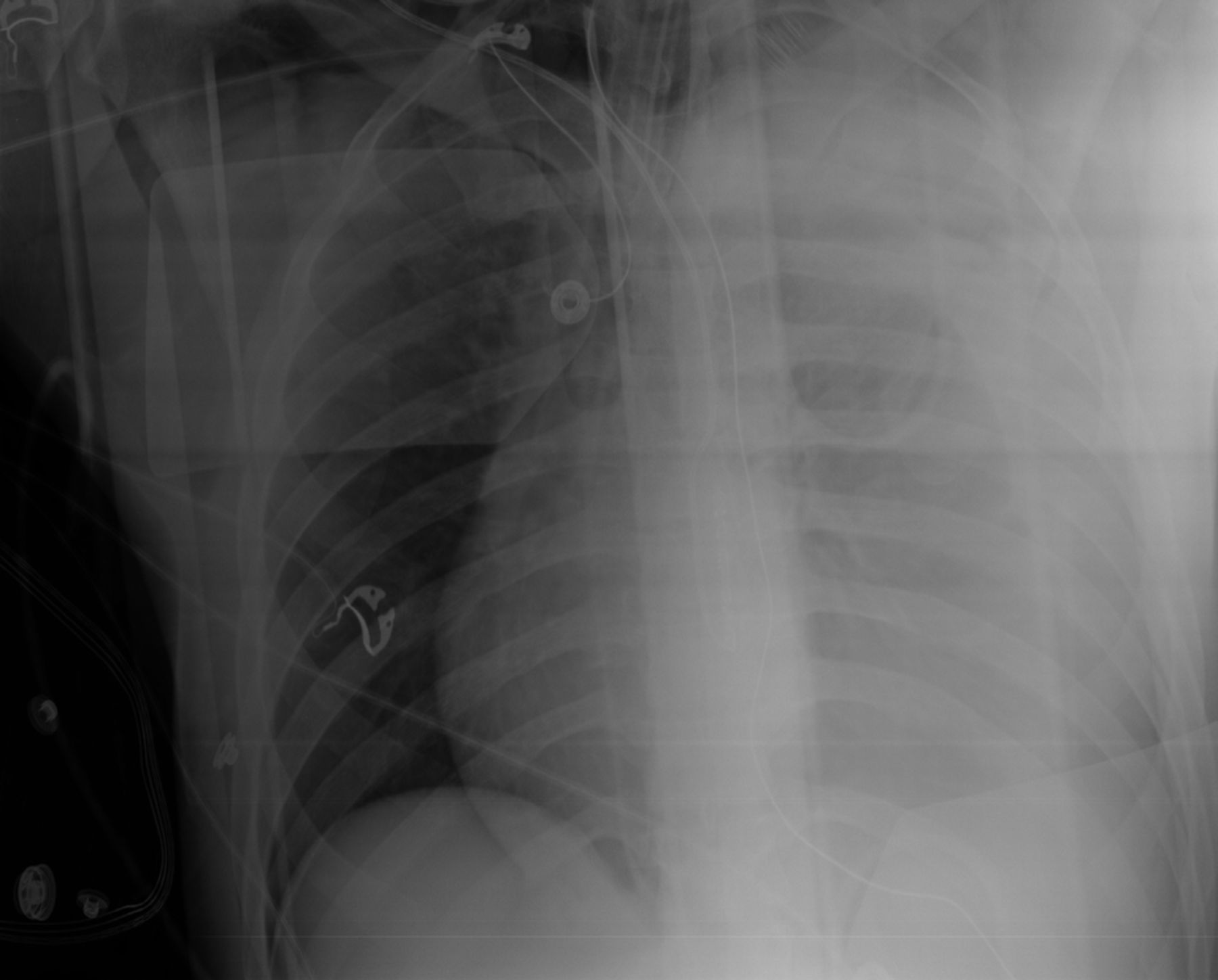
Peritoneal violation was excluded by exploration of abdominal flank wound. Total fluid replacement was—24 000 mL, 10 000 mL of crystalloids, 28 units of PRBCs, 17 units of FFP, 4 units of platelets, 4 units of cryoprecipitate. He was transferred to the trauma intensive care unit on an epinephrine drip; he was extubated on postoperative day 3, and transferred to the floor on postoperative day 6. On postoperative day 7, an echocardiogram revealed 65% ejection fraction. He was discharged home on postoperative day 13. His follow-up chest X-ray (figure 2) was normal and he has had an uneventful recovery.
{kind=link}
{kind=link}
A normal chest X-ray seen during postoperative follow-up in clinic.
Some of the teaching points that may be useful from this case are:
The choice of incision for thoracic injuries can be difficult.
Internal mammary artery injuries are rare, difficult to detect, expose, and control, and they may cause pericardial tamponade.
It is possible to explore bilateral hemithoracic cavities by incising the pleuropericardial reflection to access injured lungs.
Stapled pulmonary tractomy both central and peripheral can be used as a lung sparing procedure in 85% of penetrating pulmonary injuries.
Footnotes
Contributors JAA was involved in the conception of the manuscript. OAO contributed to the data gathering. JAA, OAO and MW were involved in manuscript writing and critical review of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/