Article Text

Abstract
An increasing number of potent antiplatelet and anticoagulant medications are being used for the long-term management of cardiac, cerebrovascular, and peripheral vascular conditions. Management of these medications in the perioperative and peri-injury settings can be challenging for surgeons, mandating an understanding of these agents and the risks and benefits of various management strategies. In this two part review, agents commonly encountered by surgeons in the perioperative and peri-injury settings are discussed and management strategies for patients on long-term antiplatelet and anticoagulant therapy reviewed. In part one, we review warfarin and the new direct oral anticoagulants. In part two, we review antiplatelet agents and assessment of platelet function and the perioperative management of long-term anticoagulation and antiplatelet therapy.
- anticoagulation
- warfarin
- antiplatelet
- reversal
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
For decades, aspirin and warfarin have been the predominant antiplatelet and anticoagulant alternatives. Beginning with the introduction of the antiplatelet agent clopidogrel in 2002, several more potent oral antiplatelet and oral anticoagulant agents have been approved for use. The increase in the number of therapeutic agents and the population at risk requires that surgeons have an understanding of the risks and benefits of reversing these agents in various settings and an understanding of the most appropriate methods for doing so. In part one of this practice management overview (in the prior issue of the journal), warfarin and the urgent reversal of warfarin-induced coagulopathy were reviewed and an overview of the newer direct oral anticoagulant agents was provided. Part two, contained herein, addresses the management of antiplatelet agents in the surgical setting, followed by general recommendations for the management of anticoagulated patients in the perioperative setting.
Antiplatelet agents
The dramatic rise in the use of endovascular stents in the treatment of cardiovascular and cerebrovascular disease has greatly increased the use of dual antiplatelet regimens to reduce acute and subacute thrombosis risk.1 The two most commonly encountered agents are aspirin (ASA) and clopidogrel (Plavix: Bristol-Meyers Squibb, New York, New York, USA). ASA's pharmacological effect on platelets is through the irreversible acetylation and inhibition of platelet cyclooxygenase-1, a critical enzyme involved in the production of thromboxane A2. The release of thromboxane A2 stimulates the recruitment and activation of further platelets and increases platelet aggregation.2 Clopidogrel is within the thienopyridine class of drugs that blocks the P2Y12 receptor on platelets for adenosine diphosphate (ADP), thus irreversibly preventing platelet activation.2 Since clopidogrel is a prodrug that requires activation by hepatic P450 enzymes, significant variability of antiplatelet activity may exist between patients. There are no specific reversal agents for clopidogrel. Since its effects are irreversible, the resultant platelet inhibition lasts for the lifespan of the platelet, ∼7–9 days.
Antiplatelet therapy in acute coronary syndrome and coronary stent placement
Current guidelines in cardiology recommend (class IA) dual antiplatelet therapy with ASA and clopidogrel for a minimum of 1 month and up to a year for patients treated medically or with bare-metal stents. For patients with drug-eluting stents, dual therapy is recommended for a minimum of 1 year.3 ,4 Cessation of clopidogrel is associated with increased risk of thrombosis in patients with acute coronary syndrome and in patients with stent placement, particularly in the first 90 days.3 Premature discontinuation of antiplatelet therapy is the strongest predictor of stent thrombosis for both bare-metal and drug-eluting stents.4–9 In one study, premature discontinuation of antiplatelet therapy resulted in a 29% thrombosis rate and a 45% mortality for patients with stent thrombosis.4 The calculated HR for all stent thrombosis (subacute and late) was 89.78 for premature antiplatelet therapy discontinuation.
Restoring platelet function
The use of antiplatelet agents has been shown to increase bleeding risks after surgery and trauma and to increase the risk of spontaneous and post-traumatic intracranial bleeding.10 ,11 However, assessing this risk is dependent on actual platelet function. Platelet counts alone demonstrate limited correlation with bleeding risk. The indications for providing agents to restore platelet function in the setting of bleeding risk are controversial.10–12 For ASA-induced platelet dysfunction, intravenous desmopressin has been shown to restore activity, though little clinical outcome data are available.10 ,13 The indications for the use of platelet transfusion to reverse the antiplatelet activity of clopidogrel and ASA have not been established and clinical data are variable.10–12 The half-life of clopidogrel is 6 hours, and thus therapeutic levels should be fairly low after 3–4 half-lives. Transfusion of platelets has been shown to reduce the antiplatelet effect, though the dosing and timing remain unclear.14 An ongoing multicenter study is currently underway to investigate the utility of platelet transfusion in cerebral hemorrhage, but no results have been published.15 Currently, to determine if platelet transfusion is indicated, an assessment of platelet function should be undertaken.
Assessing platelet function
Assessing platelet function and its contribution to bleeding risk in elective and emergent settings remains challenging, particularly with the use of aspirin or clopidogrel. Platelet activity comprises 80% of overall clot strength and the remaining 20% is determined by fibrin. As such, overall clot strength is probably best assessed using a whole blood assay rather than serum-based testing of platelet function alone. Moreover, little correlation exists between platelet count and clot strength. Patients can have normal platelet counts with markedly impaired platelet function in conditions such as von Willebrand factor deficiency and uremia. Individual tests are discussed in the sections below and summarized in table 1.
Basic characteristics and interpretation of commonly used assays to assess platelet function
Bleeding time: Although there are many tests to assess platelet function, there is no test that is readily clinically available, prospectively validated, and reliable to guide transfusion strategy or assess risk of bleeding. The bleeding time is one of the oldest tests which aimed to assess platelet function. This test involves incising the skin and blotting the hemorrhage to determine time to clot formation and arrest of bleeding. However, test results are obfuscated by differences in the amount of pressure applied. Furthermore, since the test involves making an incision, it cannot be repeated serially.
Aggregometry: This test likely represents the most accurate way to measure platelet function. However, this test is not readily available and is not portable. Aggregometry can be performed by measuring light transmittance or electrical impedance. Light transmission aggregometry (LTA) is performed by adding a known agonist, such as arachidonic acid (AA) or ADP, to a platelet rich medium.16 Note that this test is not performed using whole blood. Platelets that are stimulated by the agonist will aggregate, thereby increasing light transmission in the medium. Thus, platelet activity is directly proportional to light transmittance. Impedance aggregometry is based on the same principle as LTA but is performed on whole blood.17 This modality uses an electrical current to stimulate the platelet before and after addition of AA/ADP. Platelets that are stimulated bind to the electrodes, thereby increasing impedance. The degree of platelet inhibition due to aspirin or an ADP-receptor antagonist, such as clopidogrel, is assessed as a function of change in impedance before and after addition of the appropriate agonist. Both LTA and impedance aggregometry are best used by assessing baseline platelet function versus stimulated platelet function to determine actual versus maximal platelet activity. Unfortunately, there are no reference values (ie, normal values) to gauge the probability of bleeding.
PFA-100 and VerifyNow: Two more commonly available and more easily performed assays which also seek to measure platelet function are the PFA-100 (Siemens Medical, Malvern, Pennsylvania, USA) and VerifyNow (Accriva Diagnostics, San Diego, California, USA).18–20 PFA-100 is currently approved only to detect the presence of aspirin. This test is performed by exposing flowing whole blood to an aperture lined with epinephrine. As the platelets activate, they seal the aperture. Thus, ‘closing time’ is inversely proportional to platelet activity. VerifyNow is also a whole blood assay that is based on the principles of LTA and can detect platelet inhibition due to either aspirin or ADP-receptor blocking agents. This test is performed by placing a specimen of whole blood in a cassette that includes fibrin bonded beads. AA/ADP are added as agonists. As the beads dissolve, the fibrin interacts with the platelets and stimulates them. Light is transmitted across the cassette, and, akin to LTA, increase in light transmittance is directly proportional to platelet activity. Although both PFA-100 and VerifyNow have reference ranges regarding the degree of inhibition recommended to prevent thrombus formation, there are no validated values regarding the degree of inhibition associated with clot formation or cessation of hemorrhage.
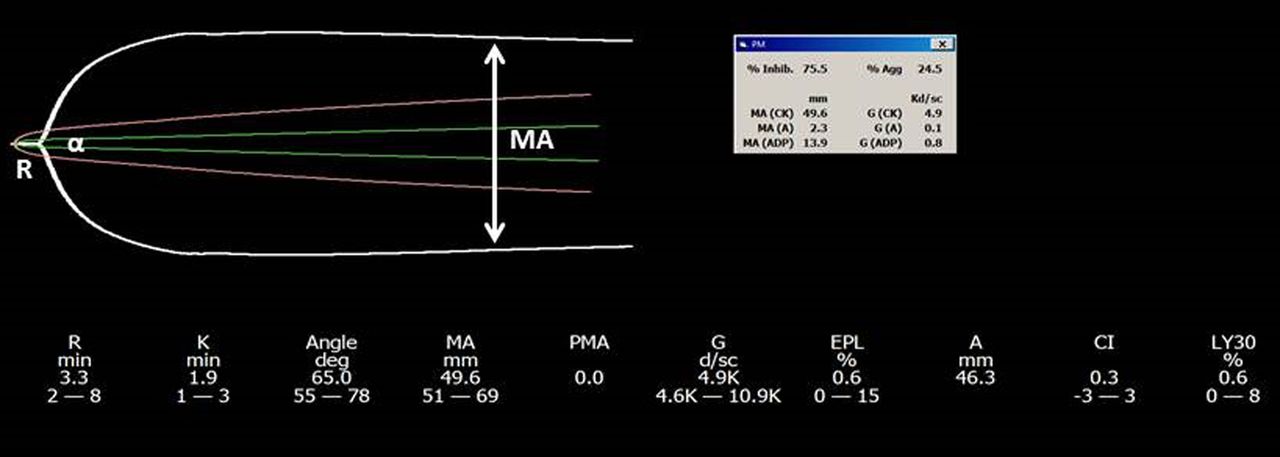
Thrombelastography-platelet mapping (TEG-PM): This test assesses platelet function using a whole blood assay.21 Blood is placed in a cup, a pin inserted, and the cup rotates. Kaolin, a clotting catalyst, is added to the specimen to start the clotting process and a graph of clot strength versus time is generated (figure 1). The maximum amplitude (MA-CK) represents the total potential clot strength, inclusive of both the platelet and fibrin component. The specimen is then re-analyzed with heparin and reptilase added. This allows measurement of the fibrin contribution to the clot (MA-F) which can then be subtracted from the MA-CK to determine the platelet contribution to clot strength. The specimen is then re-analyzed with ADP or AA added to determine the change in clot strength related to each agonist. This allows selective measurement of the degree of inhibition of platelet function due to the AA and ADP receptors, thereby quantifying the anticoagulant effect due to aspirin and ADP receptor antagonist medications (figure 2). As with the aforementioned tests, however, there are no reference ranges for the degree of inhibition associated with thrombosis or coagulopathy. Recent studies suggest that the degree of inhibition in normal volunteers is <5%, whereas the degree of inhibition can be as high as 30–60% in injured or critically ill patients.22–24 Thus, as with the other tests of platelet function, although TEG-PM is able to detect platelet dysfunction, clinical judgement is needed to apply the results appropriately in any particular scenario. Until now, there are no tests akin to the International Normalized Ratio (INR) in patients using warfarin in that no test measuring platelet function can be readily interpreted to determine the propensity for bleeding or clotting in all instances.

Standard TEG tracing. R time is reflective of enzyme/coagulation factor deficiency. α Angle is reflective of the thrombin burst. Maximal amplitude (MA) consists of 80% of platelet activity and 20% of fibrinogen. TEG, thrombelastography-platelet mapping.

TEG platelet map tracing. Note the insert which shows the degree of platelet inhibition both as a percentage of total as well as the actual MA associated with the pathway. This assay shows 75.5% inhibition in the ADP pathway. ADP, adenosine diphosphate; MA, maximal amplitude; TEG, thrombelastography-platelet mapping.
Perioperative management of long-term anticoagulation
The perioperative management of patients who require long-term anticoagulation requires careful analysis of the risk-benefit ratio, balancing the risk of thromboembolism versus the risk of hemorrhage. Determining the periprocedural risk of thromboembolism requires an understanding of the condition for which the drug is being prescribed. The most common indications include non-valvular atrial fibrillation, venous thromboembolic disease, and the presence of mechanical heart valves. Quantifying the risk associated with the specific indication for an individual patient is required to appropriately manage anticoagulation in the periprocedural period.
Assessing thrombotic risk
Thrombotic risk for individual patients varies by each of the common indications as well as by the presence or absence of individual risk factors. The methods of assessing the risks for each of the common indications are discussed below.
Non-valvular atrial fibrillation: The risk of stroke or arterial thromboembolism in non-valvular AF can be gauged by using one of a number of scoring systems, the most common being the CHADS2 or expanded CHA2DS2-VASc scores.25 ,26 For CHADS2 (see table 2), points are assigned for five risk factors: congestive heart failure, hypertension, age >75 years, diabetes, and a history of stroke, transient ischemic attack, or thromboembolism.
CHAD2 scoring system for assessing thromboembolic risk
In the expanded scoring system CHA2DS2-VASc (table 3), additional points are given for the presence of vascular disease, age between 65–74 years, and female gender.
CHA2DS2-VASc scoring system for assessing thromboembolic risk
For both systems, the annual risk of stroke increases with the total number of points (see tables 4 and 5) A score greater than two points is generally considered high risk for thromboembolism and an indication for long-term anticoagulation.25 ,26
Stroke risk by CHADS2 score
Stroke risk by CHA2DS2-VASc score
Venous thromboembolism: For a history of venous thromboembolism (VTE), patients are grouped into low-risk, intermediate-risk, and high-risk categories as outlined below.27
Low risk (<5% annual risk of VTE): a history of VTE >12 months ago;
Intermediate risk (a 5–10% annual risk of VTE): a history of VTE within 3–12 months, a ‘non-severe’ thrombophilia such as Factor V Leiden or a prothrombin gene mutation, or an active cancer (treated within 6 months or currently undergoing palliative treatment)
High risk (>10% annual risk of VTE): VTE within 3 months, or a ‘severe’ thrombophilia such as Protein C/S/antithrombin deficiency or presence of antiphospholipid antibodies.
Prosthetic heart valves: Patients with heart valve replacement are at increased risk of embolic event. Bioprosthetic valves are at much lower risk than mechanical valves and oral anticoagulant therapy is typically required only for the first 3 months after placement followed by antiplatelet therapy.28 All mechanical prosthetic heart valves require long-term anticoagulation but the risk of emboli and therapeutic targets vary depending on the valve type and position (aortic vs mitral).28 The risk of embolic event may be grouped into either intermediate or high-risk groups as determined by position, valve type, and the presence or absence of additional thrombotic risk factors.
Intermediate risk: (1) patients with aortic bileaflet or current-generation single tilting disc valves with no risk factors for thromboembolism, (2) patients with bioprosthetic valves and atrial fibrillation, atrial thrombus or enlargement, prior stroke or TIA >6 months, or with hypertension, diabetes, congestive heart failure, or age >75 years.
High risk: (1) patient with aortic caged-ball type and older generation valves, (2) any mechanical valve with atrial fibrillation, atrial thrombus or enlargement, prior stroke or TIA, congestive heart failure, and hypercoagulable conditions, (3) all mechanical valves in the mitral position.
For patients with intermediate risk, the recommended target of vitamin K antagonism anticoagulation therapy is an INR of 2.5 and for those in the high-risk group an INR of 3.0 is recommended.28
Assessing hemorrhagic risk
Remaining on anticoagulation in the periprocedural period must be balanced against the risk of periprocedural hemorrhage. While this can be difficult to quantify, the factors generally taken into account are patient characteristics and the nature of the procedure they are to undergo. Numerous scoring tools have been proposed to quantify patient hemorrhage risk including the Outpatient Bleeding Risk Index, the HEMORR2HAGES score, and the HAS-BLED score.29 ,30 The HAS-BLED score is the most commonly employed tool that has been validated to predict bleeding risk during bridging of anticoagulation.31 The HAS-BLED score assigns a point value to each of the following risk factors: hypertension, abnormal renal or liver function, stroke, bleeding history, labile INR, elderly age, and drugs (aspirin, non-steroidal anti-inflammatory drugs, alcohol) and groups patients into low, medium, and high risk of bleeding (see tables 6 and 7).
HAS-BLED score to assess bleeding risk
Risk of bleeding by HAS-BLED score
These systems can be used to gauge the risk of bleeding when considering recommendations for periprocedural management.
The nature of the procedure should also be considered when assessing bleeding risk. While there is no firm scoring system to quantify this, procedures can generally be grouped into high-risk (2–4%) and low-risk (0–2%) procedures.
High risk: cardiovascular, orthopedic, head and neck cancer or urological in nature, or those >45 min in length.
Low risk: procedures anticipated to be <45 min, cutaneous, or relatively straightforward such as a cholecystectomy.
Also to be taken into account are those situations where a small amount of bleeding can have serious consequences, such as ophthalmological procedures, or those where bleeding may not be easily detected.
After the risks of both thromboembolism and hemorrhage have been weighed against each other, the current anticoagulation status of the patient must be evaluated. It is possible to measure direct levels of dabigatran and rivaroxaban, with different recommendations for procedural timing according to plasma concentration. Patients found to have levels <30 ng/mL are generally considered safe for surgery. Those with 30–200 ng/mL are advised to delay procedures at least 12 hours if possible, followed by a recheck of plasma levels. Patients with levels between 200 and 400ng/mL should delay interventions at least 24 hours, and those with levels >400 ng/mL are considered at major risk of uncontrollable hemorrhage and should consider hemodialysis or other removal methods. However, in order to measure plasma concentrations, this requires access to mass spectrometry, which is not always readily available.
In the absence of direct level measurements, estimates can be obtained with other qualitative estimates or indirect quantitative measurements. Warfarin can be quantitatively estimated with INR measurement. Direct thrombin inhibitors such as dabigatran can be qualitatively estimated using activated partial thromboplastin time, prothrombin (PT), or thrombin time or quantitatively measured with dilute thrombin time, ecarin chromogenic assay, or ecarin clotting time. Factor Xa inhibitors such as rivaroxaban or apixaban can be estimated via PT or measured with chromogenic antifactor Xa. Antiplatelet agents are gauged qualitatively with optical aggregometry or quantitated with flow cytometry, platelet function assay, or thromboelastography. While these tests can give an estimate of the patient's current status, they are far from exact and can only serve as an indicator of anticipated complications in the event of an emergency, although they may be useful in attempting to reduce risks in semiurgent or elective cases.
Management of anticoagulation in elective cases
Three factors that need to be considered in the case of elective surgeries are (1) when to stop, (2) whether to bridge, and (3) when to restart.
Discontinuation prior to surgery: General recommendations are summarized in the table (table 8) below and are according to the American College of Chest Physician 2012 Guidelines published in Chest, the RE-LY trial published in Circulation 2012, the ROCKET AF trial, and the manufacturer's recommendations.32–35
Recommendations for timing of discontinuation of anticoagulation for elective surgery
Patients whose procedures are at low risk of bleeding may continue oral anticoagulation therapy. This is particularly true for high-risk patients such as those with mechanical heart values.
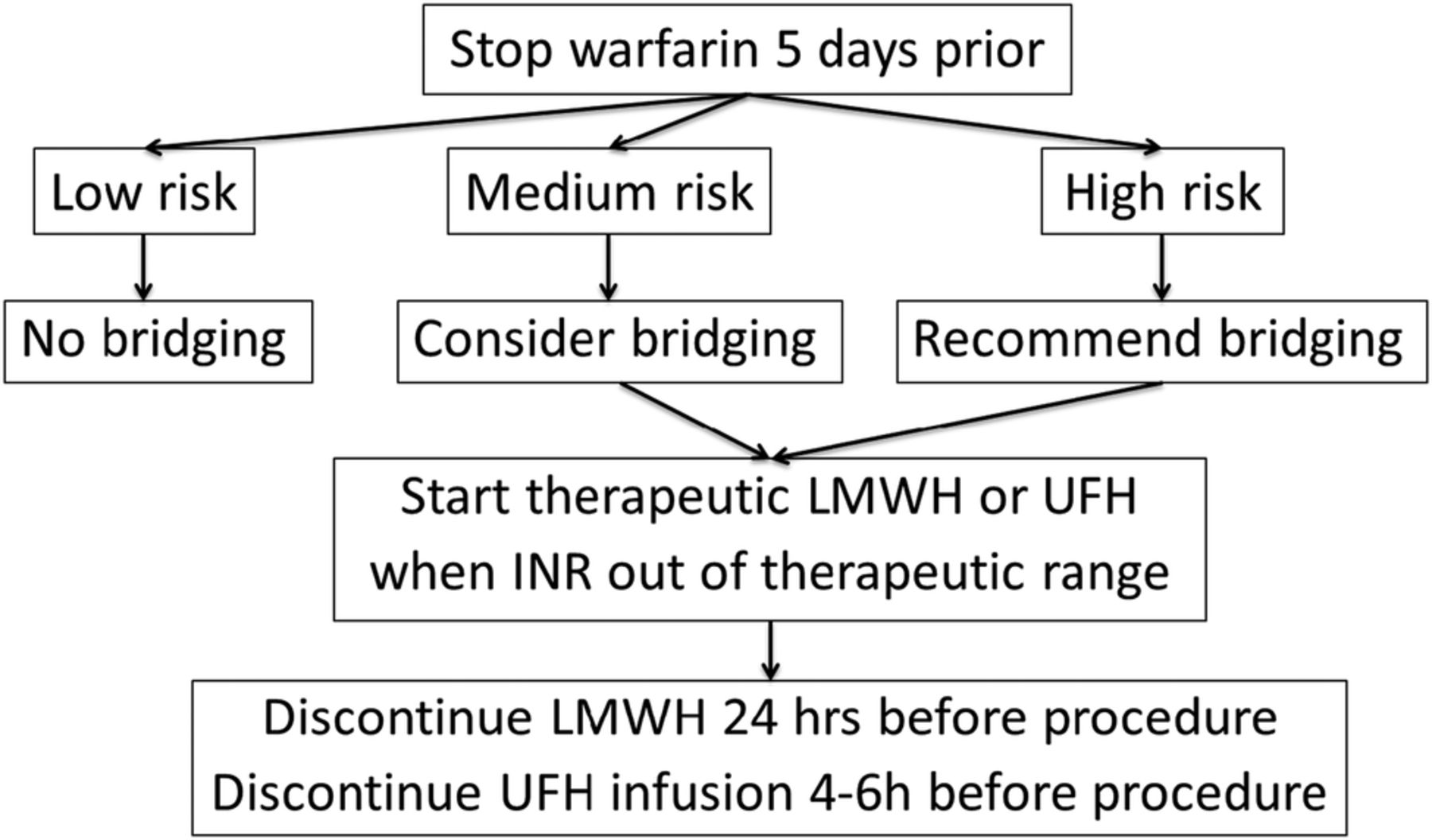
Indications for bridging: The need for perioperative bridging is decided on by taking into account the patient's thromboembolism and hemorrhage risk and stratifying them into low, medium and high risk. In the case of warfarin, recommendations are summarized in the flow chart below (figure 3), adapted from the 2012 American College of Chest Physicians Guidelines.32 Bridging may be achieved either with intravenous unfractionated heparin or with subcutaneous low-molecular-weight heparin. Temporary interruption of vitamin K antagonism agents, without bridging while the INR is subtherapeutic, is recommended for patients with bileaflet mechanical aortic valve replacements and no other risk factors.28 All other mechanical valve settings should undergo bridging.
{kind=link}
{kind=link}
{kind=link}
Algorithm for perioperative bridging of warfarin. INR, International Normalized Ratio; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin.
Efficacy of bridging: Whether or not outcomes are really better with bridging patients on vitamin K antagonists remains uncertain. A meta-analysis published by Siegal et al35 in 2012 found that the rate of thromboembolism was equivalent in patients who underwent periprocedural heparin bridging; however, there was a significantly higher number of patients who had major bleeding complications in those undergoing heparin bridging. These results were replicated in a randomized controlled trial by Douketis et al36 in 2015 demonstrating non-inferiority between patients undergoing no bridging versus those with low-molecular-weight heparin bridging and a significant reduction of major bleeding complications in those patients who did not undergo bridging.
With the non-vitamin K antagonist oral anticoagulants, no strong evidence to support bridging exists currently. These anticoagulants have a shorter half-life and faster onset making the benefits of bridging less obvious. A study from the European Dresden registry from 2014 demonstrated that in patients taking nonvitamin K antagonists, heparin bridging did not reduce cardiovascular events, and major bleeding again was more frequent with bridging than without.37 Additionally, the HASBLED scoring system used to gauge the risk of hemorrhage can also be used to estimate risk of hemorrhage heparin bridging during warfarin cessation.31 Recommendations are unclear regarding the efficacy and need for bridging with DOACs.
Re-initiation of oral anticoagulation: The decision to restart anticoagulation after a procedure is again determined by weighing the risks for thromboembolism against that of hemorrhage. If hemostasis is assured after the procedure, vitamin K antagonists can be restarted 6–24 hours after surgery as therapeutic levels will take several days to reach. If periprocedural bridging is being used, patients at low risk of bleeding can resume bridging at 24 hours and those at higher bleed risk at 48–72 hours for all high-risk patients. Non-vitamin K antagonists could potentially be resumed after 6–24 hours in patients with low bleeding risk if hemostasis is assured, bearing in mind that these agents have a much faster time of onset. Those with higher bleeding risk should wait 48–72 hours prior to restarting and could be considered for bridging with heparin if the risk of thromboembolism is also high.
Management of anticoagulation in urgent/emergency cases
In cases where future planning and weighing risks and benefits for periprocedural management cannot be accomplished, the two main goals are initial management of anticoagulation followed by employment of reversal strategies. Initial actions include discontinuing the anticoagulant, delaying semiurgent procedures as appropriate, and consideration of activated charcoal for ingestions <2 hours prior.
Several reversal strategies in the urgent/emergent setting for anticoagulant and antiplatelet therapies agents are summarized below and reviewed in previous publications.38
Antiplatelet agents: Current recommendations suggest that patients with active bleeding or at high risk of bleeding and those who have platelet counts <50 000/µL undergo platelet transfusion.38 Antiplatelet therapy has been shown to worsen the outcome of patients with intracranial hemorrhage or traumatic brain injury.10 ,11 However, the indications for platelet transfusion to restore platelet function remain controversial.10–12 Some authors and guidelines recommend transfusion of 5–10 units of platelet concentrates in patients with intracranial hemorrhage receiving antiplatelet therapy.38–40 However, the efficacy of platelet transfusion in the setting of non-reversible antiplatelet agents is not fully established, although research is currently ongoing.15 There may also be some role for desmopressin in the setting of ASA therapy, although indications have not been well elucidated.10 ,13
Vitamin K antagonists: The first-line Food and Drug Administration (FDA)-approved strategy is the intravenous infusion of vitamin K, 1–10 mg intravenous over 30 min, followed by prothrombin complex concentrates (KCentra) 25–50 units/kg as second-line therapy. A third-line strategy is fresh frozen plasma for an INR >2. Recombinant factor VII remains as an option, although this is currently not approved by the FDA.
Direct thrombin inhibitors: dabigatran is the most commonly prescribed direct thrombin inhibitor. Idarucizumab, a specific antibody reversing agent, is now approved for use as the first-line reversing agent for Dabigatran. First-line recommendations consist of Factor VIII Inhibitor Bypassing Activity (FEIBA) 50–100 units/kg, followed by PCCs 25–50 units/kg as a second-line option. Recombinant Factor VII can be used as a 100 µg/kg bolus, repeated as needed. Hemodialysis can also be effective in clearing direct thrombin inhibitors from the bloodstream.
Factor Xa inhibitors: First-line reversal agents are 4 factor PCCs 25–50 units/kg followed by FEIBA 50–100 units/kg (with a maximum dose of 200 units/kg daily) as a second-line agent. Target-specific agents such as andexanet α and PER977 are also in the process of undergoing development and testing.
Management of antiplatelet therapy in the perioperative period
Inadequate data are available to establish firm recommendations regarding cessation or continuation of antiplatelet therapy in the elective or urgent perioperative setting. The risks of bleeding and outcomes from bleeding must be weighed against the thrombotic risks and substantial associated mortality.3–9 Studies of bleeding risk have provided conflicting information. One randomized study involving only 52 patients receiving ASA did not find a significant difference in the incidence of perioperative hemorrhage in patients undergoing cholecystectomy, colorectal surgery, or inguinal hernia repair.41 Patients in this study were randomized to stop aspirin for 5 days before and after operation versus continuing aspirin throughout the perioperative period. A number of retrospective and prospective cohort studies have examined the risk of bleeding with dual antiplatelet therapy with disparate results.42 A recent systematic review found no difference in the incidence of bleeding in gastrointestinal surgery when all studies were considered.42 Of the various studies performed, only one involved pancreatectomy, five involved cholecystectomy, and eight involved endoscopic polypectomy. The largest study involving general surgery patients included 1075 patients and similarly did not find a significant difference in the probability of bleeding related to ongoing use of single antiplatelet agents following various laparoscopic operations.43 However, use of dual antiplatelet agents was associated with a higher rate of hemorrhage in multivariable analysis. In total, there is insufficient evidence on which to base a recommendation regarding perioperative management of antiplatelet therapy. Clinical discretion is needed to weigh the risk of bleeding versus the risk of thrombosis.
References
Footnotes
Presentation: Portions of this review were presented at the 2015 Clinical Congress of the American College of Surgeons, 7 October 2015, Chicago, Illinois, USA.
Contributors All authors had substantial contributions to the writing and editing of the article.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.