- 1University of Massachusetts Medical School, Worcester, Massachusetts, USA
- 2Division of Trauma and Critical Care, University of Massachusetts Medical School, Worcester, Massachusetts, USA
- 3Department of Surgery, University of Massachusetts Medical School, Worcester, Massachusetts, USA
- Correspondence to Dr Jon D Dorfman; jon.dorfman{at}umassmemorial.org
- Received 26 May 2016
- Revised 24 June 2016
- Accepted 27 June 2016
- blunt trauma
- bowel injuries
- herniation
- Motor vehicle trauma
A 43-year-old woman was the driver in a car crash versus a tree. After a prolonged extrication, she was taken to a local community hospital. Her injuries on clinical examination included an abdominal wall defect with small bowel evisceration and multiple orthopedic extremity injuries. She was intubated at the community hospital for altered mental status. The patient was then sent by air transport to our level I trauma center for further management. On arrival at the trauma bay, 3 hours after the injury, her pulse was 125 bpm and her blood pressure was 100/56 mm Hg. Her Glasgow Coma Scale was 3 T during the initial trauma bay assessment. Physical examination was notable for a left lower quadrant laceration that revealed an eviscerated small bowel.
What would you do?
Perform abdominal imaging and close the defect if no intra-abdominal injury is detected?
Proceed to the operating room (OR) for prompt exploratory laparotomy and surgical repair with or without mesh?
Proceed to the OR for exploratory laparotomy and component separation repair of the abdominal wall?
What we did and why
Correct answer: B
CT scans of the head, cervical spine, chest, abdomen and pelvis (figure 1) were performed to determine if intracranial hemorrhage, aortic injury or cervical and thoracolumbar spine injuries were present. No additional injuries were detected on imaging.
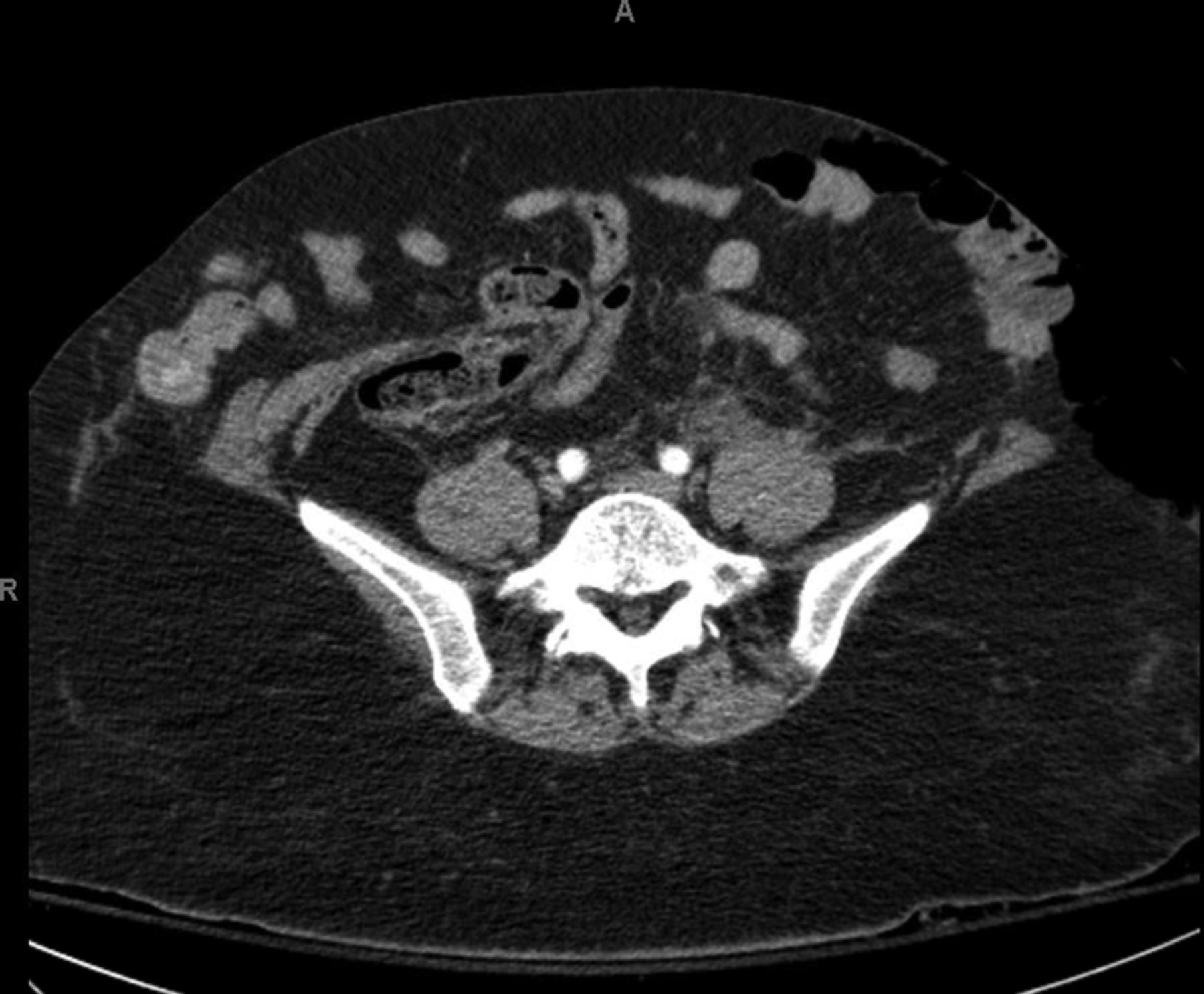
A cut from a preoperative abdominopelvic CT scan.
The patient was then taken to the OR for abdominal exploration and staged surgical repair of the abdominal wall defect. The left lower quadrant abdominal wall laceration measured 25 cm in length. The wound tracked through the subcutaneous tissue toward the midline; the external and internal oblique muscles were disrupted on the left but the peritoneum and transversus abdominus was intact. In the midline, a 20×15 cm full-thickness abdominal wall defect was noted. No hernia sac was identified, suggesting an acute traumatic rupture of the abdominal wall, and not that of a pre-existing hernia with laceration. The wound tracked to the right lower quadrant, but here the superficial skin and the deeper muscular layers of the abdominal wall were intact and there was a separation of the fascia from the overlaying soft tissue (figure 2A). The traumatic skin laceration was then extended by 15 cm to the midline and the abdominal viscera were examined through the traumatic 20×15 cm fascial opening (figure 2B). Exploration of the peritoneal cavity revealed only a tear of the mesentery of the sigmoid colon without active bleeding or compromise of the associated bowel. The abdomen was then washed out. The devitalized skin and subcutaneous fat were debrided from the traumatic wound. A partial complex closure of the abdominal wall was then performed. The left lower quadrant external and internal oblique were reapproximated after releasing the fascia from the overlaying soft tissue to reduce tension. Complete closure of the abdominal wall was not possible at that time due to tissue loss, rectus muscle retraction, and the patient's worsening metabolic acidosis. As a result, the omentum was pulled down over the defect to protect the underlying bowel and negative pressure wound therapy placed. Two days later, the patient was taken for abdominal wall reconstruction using biological mesh. The left lateral aspect of the overlying skin and subcutaneous tissue developed necrosis and subsequently required surgical debridement. The wound eventually healed by secondary intention with wound vacuum assistance. At 7 months follow-up, the patient had a completely healed abdominal wall, no sign of abdominal hernia and had returned to preinjury activity status.
{kind=link}
{kind=link}
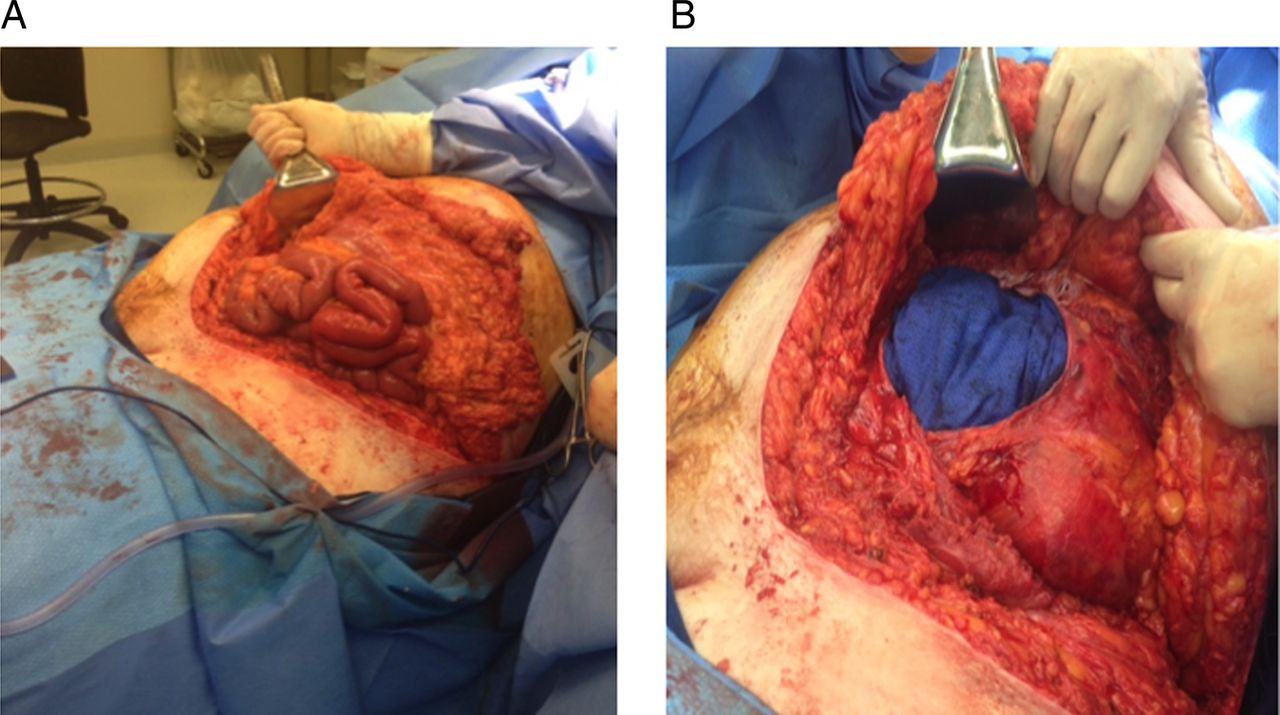
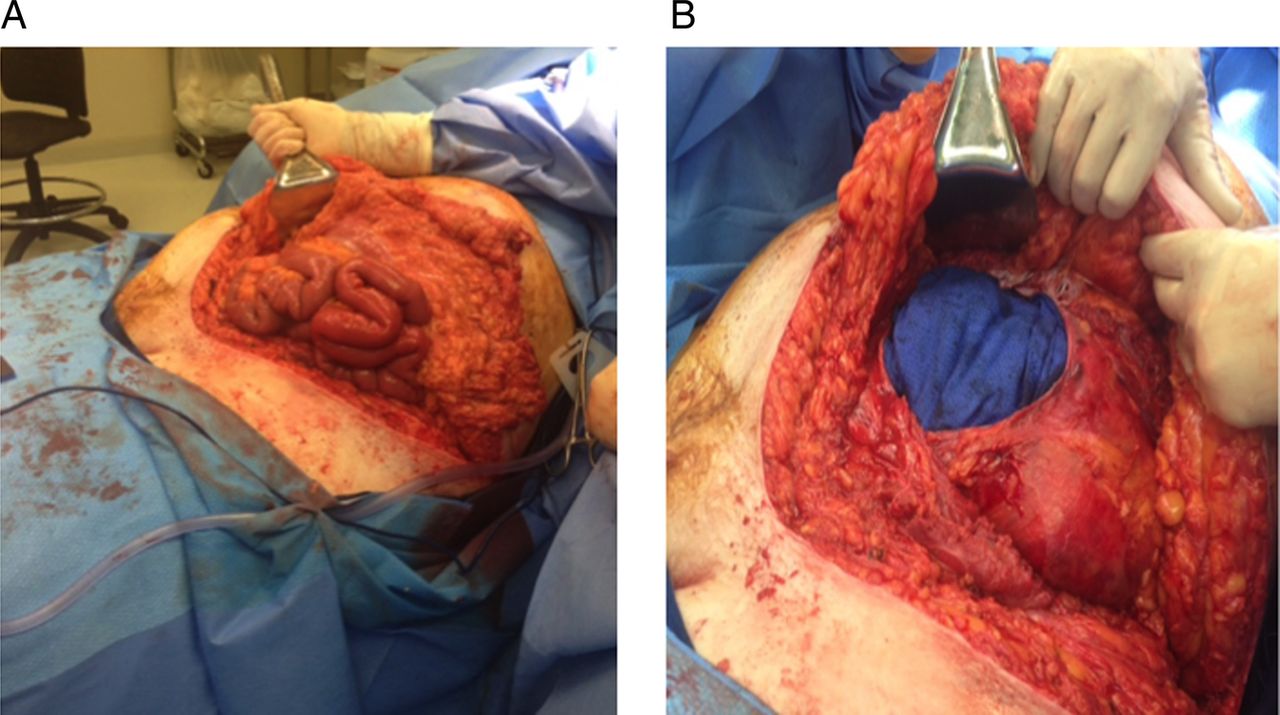
Intraoperative images depicting the traumatic abdominal wall defect with evisceration of the bowel (A) and the surgical extension of the skin laceration by 15 cm to the midline, allowing for the further exploration of the abdominal viscera (B).
Blunt trauma resulting in disruption of the abdominal wall, also known as traumatic abdominal wall herniation (TAWH), is an infrequent event. TAWH with evisceration is even less common with an estimated incidence of 1 in 40 000. TAWHs are thought to result from severe blunt trauma, which disrupts the fascial layers and the abdominal wall musculature through a simultaneous surge in abdominal pressure and shear force. This report describes the presentation and management of a case of TAWH with abdominal evisceration following a motor vehicle crash. Abdominal exploration and staged surgical repair of the abdominal wall defect were performed, with a positive clinical outcome.
Prompt surgical evaluation and repair is required in TAWH with abdominal evisceration. In addition to repairing the TAWH, exploratory laparotomy should be considered to look for associated injuries that may not be detected on CT scan, such as hollow viscous injuries. Repair of the abdominal wall defect may be accomplished by either mesh and/or primary repair. If immediate reconstruction of the abdominal wall is not possible, as is the case in this report, a staged abdominal wall closure may be performed. Owing to the high risk of infections in these contaminated wounds, synthetic mesh should be avoided. In cases such as ours, where there is tissue loss, the use of biological mesh may be required. Alternatively, abdominal wall reconstruction with component separation could be considered in the non-acute setting once the patient is no longer in the acute phase of their illness. Long-term follow-up is required to ensure that the patient has satisfactory outcomes without hernia occurrence.
Footnotes
Contributors MGN was involved in writing the manuscript. RND and JDD were involved in surgical management of patient. MGN, RND and JDD were involved in manuscript proofreading and revisions.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/