Article Text

Abstract
Rib fractures are among the most common traumatic injury found in ∼20% of all patients who suffer thoracic trauma. The majority of these are a result of a blunt mechanism and are often associated with other traumatic injuries. The most common associated injury is lung contusion. Rib fractures impart an increased morbidity and mortality with the highest mortality associated with a flail chest in the elderly population. Flail chest is defined radiographically as 3 or more consecutive ribs fractured in 2 or more places. This often translates to a clinical flail which is associated with paradoxical chest wall movement during respiratory cycles. The mainstay of treatment has been pain control and respiratory support with positive pressure ventilation. However, over the past 2 decades, there has been mounting evidence to suggest that open reduction and internal fixation of ribs benefits patients. The indications remain confined to the most severely injured patients with flail chest or chronic non-unions; however, there remains debate whether or not less severely injured patients would benefit as well. This article will review the current evidence and provide proposed indications based on available evidence and current expert opinion.
- Ribs
- rib fractures
- Chest wall
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Rib fractures are injuries that have interested healthcare professionals as far back in history as the Edwin Papyrus 1600BCE. Of the 48 cases described in this ancient text, three directly refer to chest trauma/rib fractures. Rib fractures have been reported to occur in 20% of patients with thoracic trauma. They are the most common thoracic injury and occur usually after blunt trauma. Rib fractures are responsible for significant loss of work days and can affect patients for several months after the injury.1
Rib fractures are often associated with other traumatic injuries including lung contusion, hemothorax, pneumothorax, and blunt cardiac injury. In the elderly population whose bones are more brittle we see a higher incidence of rib fractures and higher morbidity/mortality. Those patients with flail chest, defined as a contiguous segment of three or more ribs with two or more fractures, have a significantly higher mortality and respiratory failure. Flail chest can be a radiological flail as defined or a clinical flail which adds the paradoxical movement of flail segment with respirations. It is often the underlying lung contusion that leads to respiratory failure but pain and splinting leading to worsening atelectasis is also a major contributor to respiratory compromise. Therefore, pain control has been a pivotal management strategy for those with rib fractures in an effort to improve respiratory mechanics.
In the 1950s, there was greater interest in open reduction and internal fixation; however, positive pressure ventilation technology had improved becoming the management strategy for severe rib fractures. This positive pressure ventilation became ‘internal fixation’ and served as the primary management for those patients with rib fractures/flail chest with respiratory failure. Paris et al2 in 1975 published a study which demonstrated benefit in those with flail chests who were on mechanical ventilation. This small study sparked the debate and led to another study using Kirschner wires for fixation in 1979.3 As the technology of internal fixation devices improved in the 1980s and the biomechanical properties of ribs and the effect of repair on pulmonary mechanics4 was better understood,5 surgeons began to reinvigorate the effort to perform open reduction internal fixation (ORIF) on severe rib fractures. The literature began to grow regarding rib fixation and over the past decade has increased 10-fold (figure 1).

Number of articles related to rib fixation on PubMed as of March 1, 2017.
Various surgeons (trauma, orthopedic, thoracic) have increasingly fixed ribs; however, consensus regarding the indications, technique, and timing remains elusive. Some have suggested that this treatment modality is underused overall.6 One published survey found 26% of thoracic/orthopedic/trauma surgeons who thought a patient needed a repair had experience with the literature or how to perform the repair.7 This review will focus on the current literature regarding rib fixation and offer possible indications to guide surgeons.
Current trials
There are a number of prospective8 and retrospective9–14 small trials with six ongoing trials listed on clinicaltrials.gov. The three randomized trials regarding rib fixation shared similar inclusion criteria and similar results. A first randomized clinical trial was carried out by Tanaka et al15 in 2002. They enrolled patients with the following inclusion criteria: >5 ribs fractured with flail chest and mechanically ventilated for at least 5 days. A total of 37 patients were enrolled and randomized to repair with Judet struts or treated solely with mechanical ventilation and were weaned as tolerated. The outcome measures were intensive care unit (ICU) length of stay, pneumonia, and need for tracheostomy. The long-term outcome measures included return to work at 6 and 12 months. They demonstrated a significant decrease in pneumonia (22% vs 90% at 21 days), decrease in time on mechanical ventilation (10.8 vs 18.3 days), decrease length of stay in ICU by a week, and significant decrease in need for tracheostomy. The forced vital capacity was significantly increased in those surgically repaired and return to work had dramatically increased at 6 and 12 months.
The second randomized clinical trial was carried out by Granetzny et al16 in 2009. They included all patients with a flail chest and randomized 40 patients to either surgical repair with Kirschner wires or conservative treatment with chest wall stabilization with an adherent dressing over the flail segment. The results favored the surgical fixation group with a significant decrease in chest infections and chest wall deformity with significant increase in pulmonary function tests.
The third randomized clinical trial was carried out by Marasco et al17 in 2013. They enrolled those with flail chest who were mechanically ventilated and randomized 46 patients to either fixation with absorbable plates or non-surgical management. Again the results favored surgical management with a significant decrease in ICU length of stay (285 vs 359 hours), need for tracheostomy, and a trend towards a lower rate of pneumonia (48% vs 74%). Although these trials have their limitations, they provide a clear message that patients who require mechanical ventilation with a flail chest benefit from surgical fixation. The optimal method of fixation is not clear as there have been no studies comparing fixation techniques.
Indications
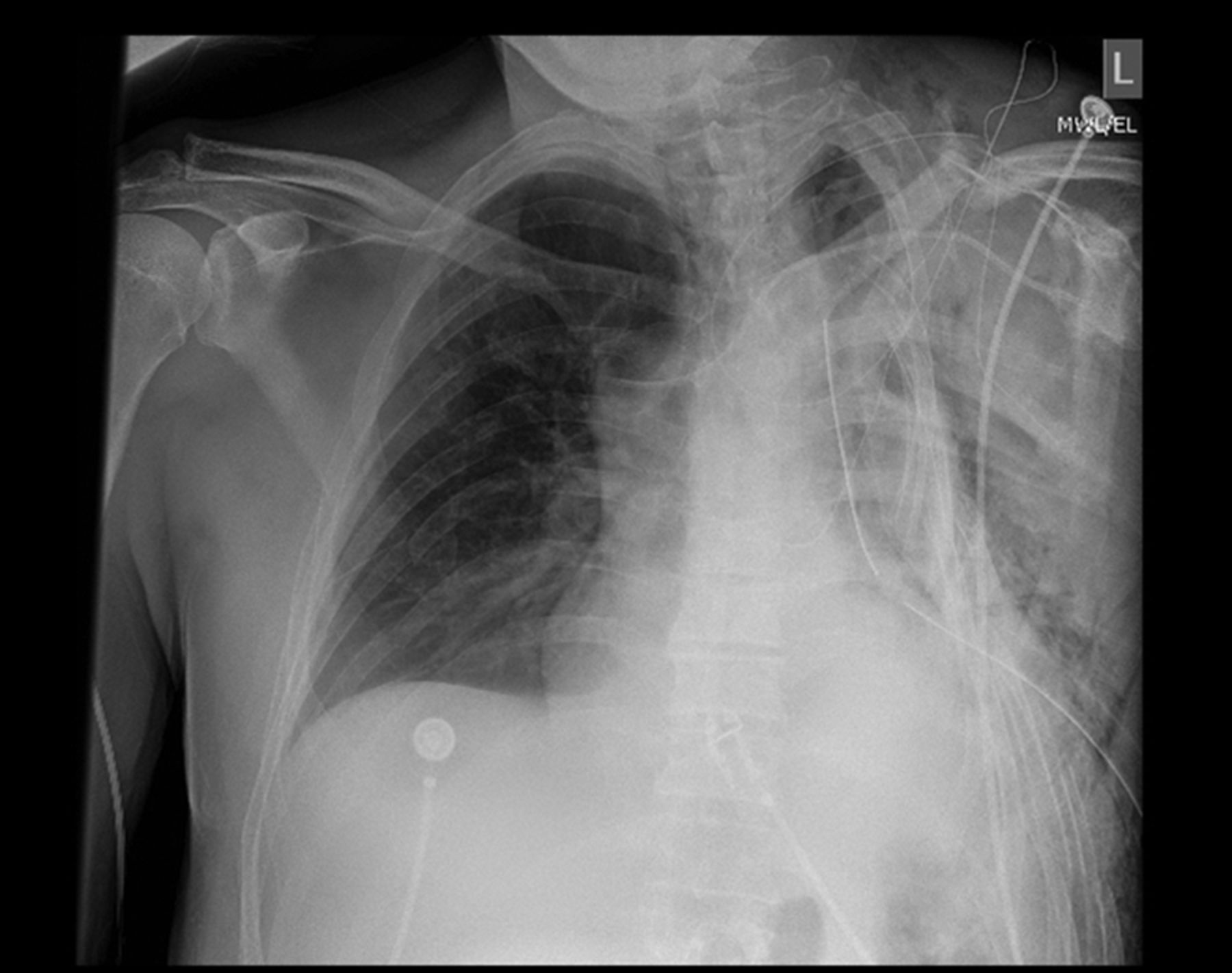
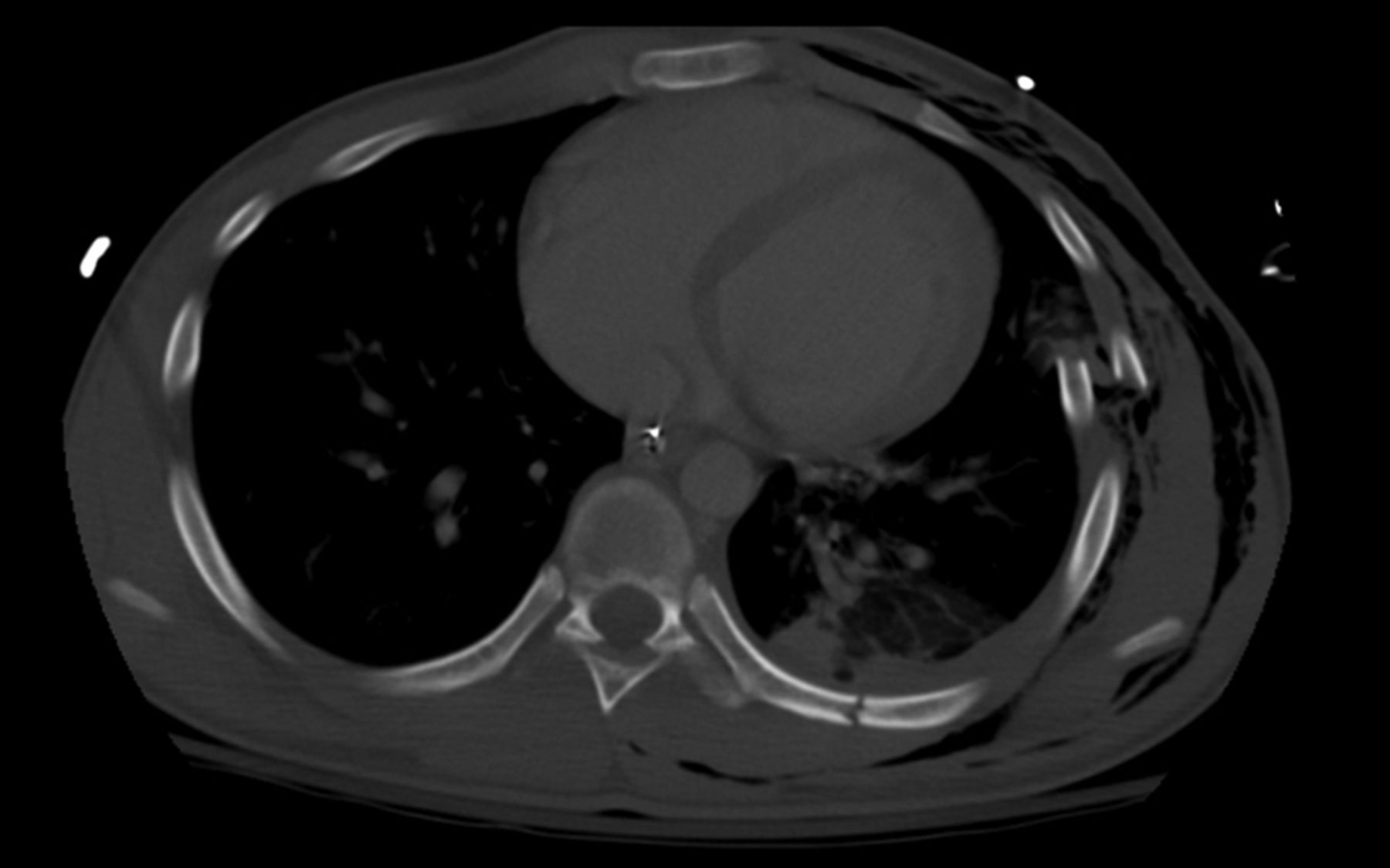
After review of the current studies, it is recommended that one should consider fixation for those with five or more ribs fractured with a flail (see figures 2⇓–4), particularly those requiring invasive or non-invasive positive pressure ventilation. The caveat to this are those patients who will require long-term mechanical ventilation for other reasons, for example, severe traumatic brain injury, high cervical cord injury or severe underlying lung disease. The use of pain severity score as a criterion for fixation has been called into question, as pain is a subjective and variable from patient to patient.18 However, pain not relieved adequately with medical treatment in addition to respiratory compromise (eg, deficiency in pulmonary function tests) may be reasonable. There are a number of retrospective and prospective observational studies that also support other indications for surgery: symptomatic non-union,19 chest deformity, and thoracotomy for other reasons (box 1).
Indications
Recommended:
≥5 rib flail chest requiring mechanical ventilation;
Symptomatic non-union;
Severe displacement found during a thoracotomy for another reason.
Consider:
≥3 rib flail not requiring mechanical ventilation;
≥3 ribs with severely displaced fractures (bi-cortical displacement);
≥3 ribs with mild to moderate displacement and 50% reduction of expected forced vital capacity percent despite optimal pain management.
Absolute contraindications:
Contaminated field.
Relative contraindications:
Severe lung contusion requiring prolonged mechanical ventilation;
High cervical spine injury requiring mechanical ventilation.
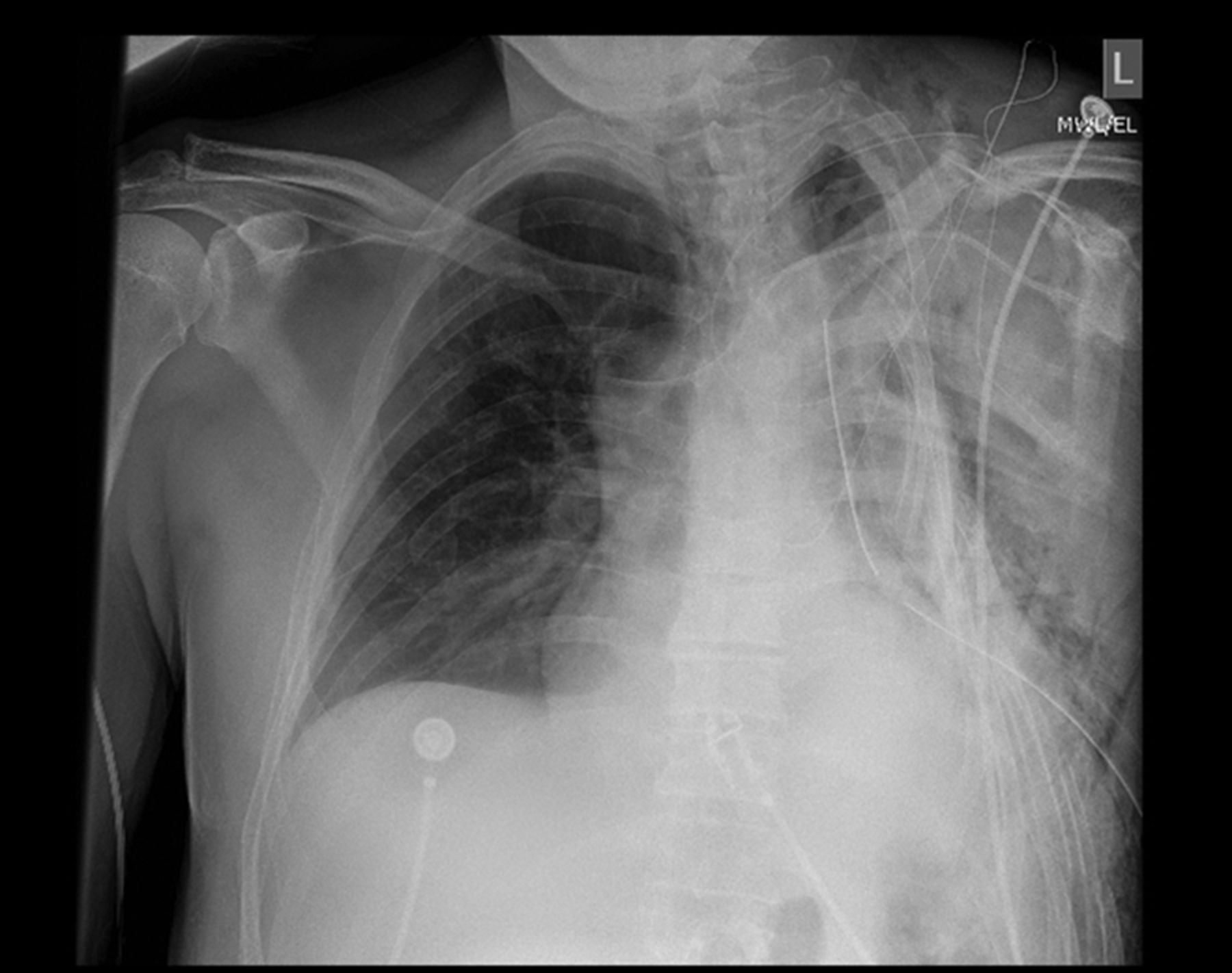
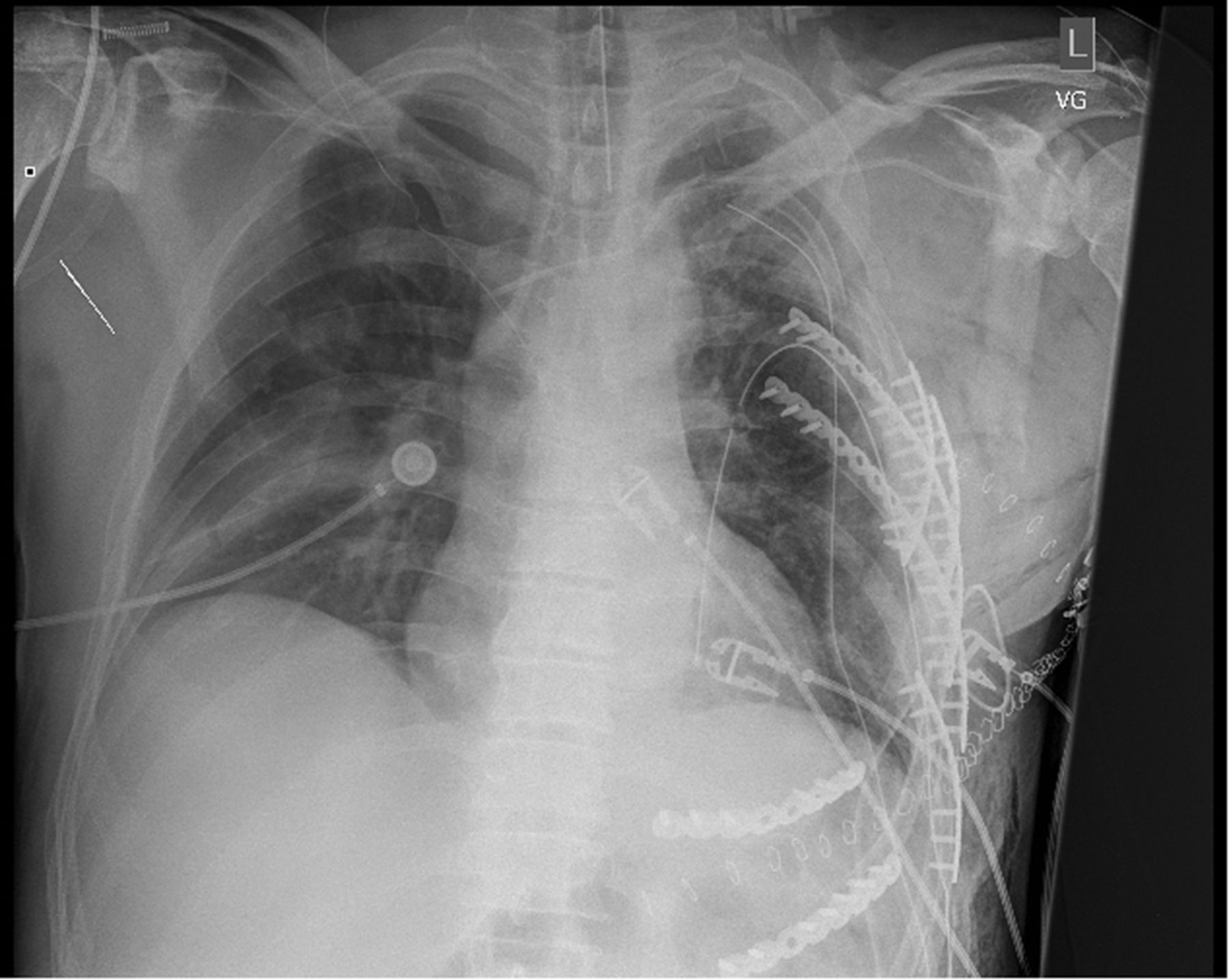
Chest X-ray with severe chest wall injury.

CT axial imaging of severely injured chest wall.

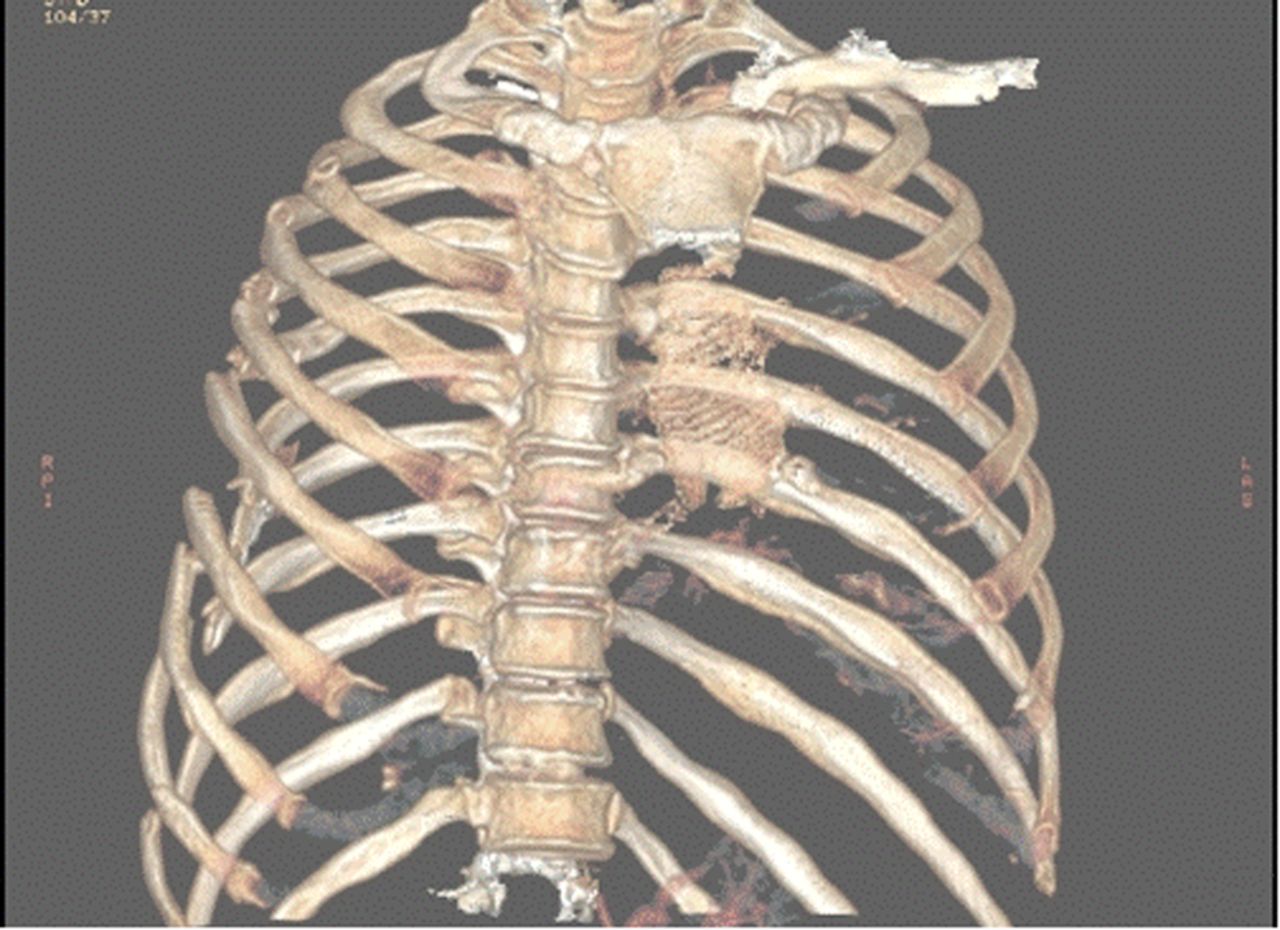
Three dimensional reconstruction of severely injury chest wall.
Technical considerations
Once a patient is identified preoperative, CT scan is helpful to plan the incision and to decide on the best course of action (figures 3 and 4). There are a number of devices available which predominately fall into five categories: (1) plating with cortical screws (single plate or U-type plate20), (2) absorbable plating,21 ,22 (3) Judet struts or Judet-like struts, (4) Kirschner wires, and (5) intramedullary rods. The majority of studies use plates with cortical locking screws. There are no studies that suggest one device being superior to another. Once the patient is identified and the device decided on one must assess the position of the rib fractures via the CT scan which can also provide a three-dimensional illustration (figure 4). These reconstructions can be helpful for operative planning.
The most common ribs repaired are the 4th through the 10th. These are the most mobile ribs and produce a significant amount of pain. The first through third ribs are more difficult to access and the benefit of the added dissection/trauma may not justify repairing these ribs; however, there is no high level evidence to suggest no benefit. There is some evidence to suggest that not all the fractures on multiple levels need to be repaired.23 Therefore, we recommend that if those ribs are severely displaced and accessible from the main incision, then it is reasonable to attempt the repair. If the fractures are anterior, the patient may remain supine, however, if the fractures have a lateral or posterior component, then a lateral decubitus position is preferable.
The incision should be minimized by strategically placing the incision in the middle of the segment to be repaired (figure 5). One should remember that the posterior chest wall may be more easily accessed via the auscultory window. A skin flap should be raised in order to allow for maximal movement of the incision to visualize the necessary muscular windows. Dissection is carried out to allow access to the rib segment but should be minimized and muscle spared. The periosteum of the rib should remain in place and not excessively dissected. When using plates, there should be just enough space to reduce the fracture and find a landing zone for the screws (figure 6).

Intraoperative image of rib plating of chest wall.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postoperative chest X-ray following rib fixation with plates.
Often the pleura has been violated by the initial trauma and therefore entrance into the pleura is common. It is our recommendation that the pleura is entered in a location central to the segment to be repaired so as to ensure full reduction of the ribs and to protect underlying lung from the drill and screws of the plates. This also allows any remaining hemothorax to be evacuated from the chest and a chest tube placed. At times, it is also to the patient's benefit to perform a video-assisted thoracoscopy to ensure the lung is fully inflated, to inspect the diaphragm, and to ensure full evacuation of any remaining hemothorax. Some also advocate the use of bronchoscopy to ensure clearance of secretions and testing of sputum for bacteria. If the bronchial lavage is positive for bacteria, some advocate a course of antibiotics to help prevent infection of the hardware. At the conclusion of the operation, a chest tube or chest drain (ie, Blake drain) may be placed and should be removed in the first 24–48 hours.
Postoperative complications
The most common postoperative complications are related to the underlying injuries, that is, lung contusion. However, there are instances of hardware infection in ∼1–3% of patients. In these cases, it is important to drain any empyema, initiate antibiotics, and after decreasing bacterial count remove the hardware. If the fracture site is well healed, one may remove the hardware at the first signs of trouble. This is an uncommon complication but requires a multimodality approach.24 Retained hemothorax or persistent air leak must be monitored with postoperative imaging.
Conclusions
Rib fractures are the most common blunt thoracic traumatic injury. The treatment of rib fractures begins with adequate analgesia and may necessitate open reduction internal fixation. Minimally invasive techniques to reduce and fix ribs are on the horizon.
References
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.