Article Text

Statistics from Altmetric.com
Surgical dilemma
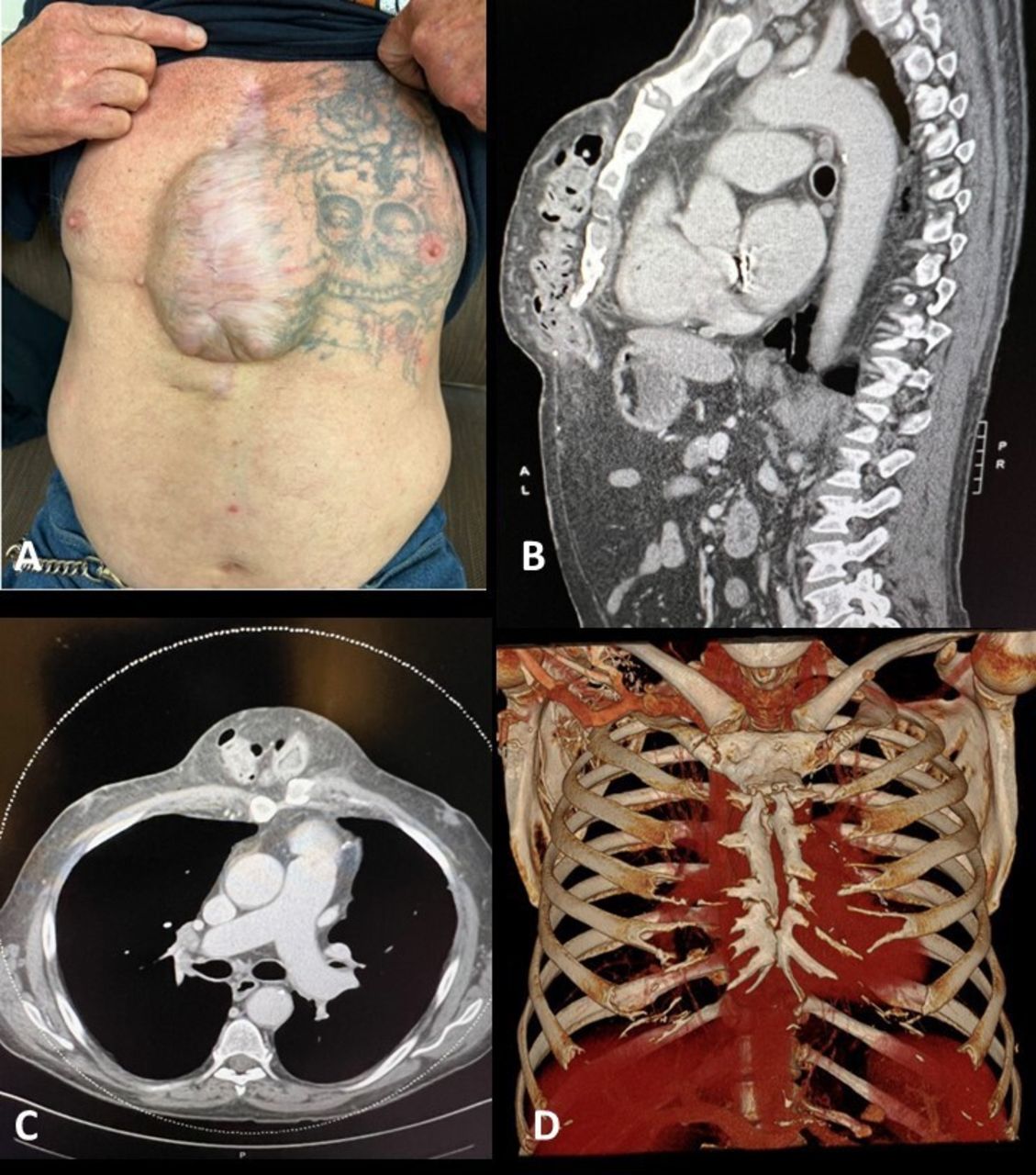
A man in his 60s presented to the emergency department with a painful chronic midline bulge in the upper abdomen and lower chest (figure 1A). During the past few months, he had sought care many times at multiple regional hospitals for the same issue. Two years prior, he had undergone a sternotomy for coronary artery bypass graft and mitral valve annuloplasty, which was complicated by methicillin-resistant Staphylococcus aureus mediastinitis requiring sternal debridement. The bulge had developed after surgery and had increased in size over time. He also reported worsening constipation. The 2×8 cm bulge was tender on examination without any overlying skin changes. CT showed chronic sternal non-union with absent xiphoid process (previous resected), and transverse colon herniating through a subxiphoid fascial defect without evidence of strangulation or obstruction (figure 1B–D).
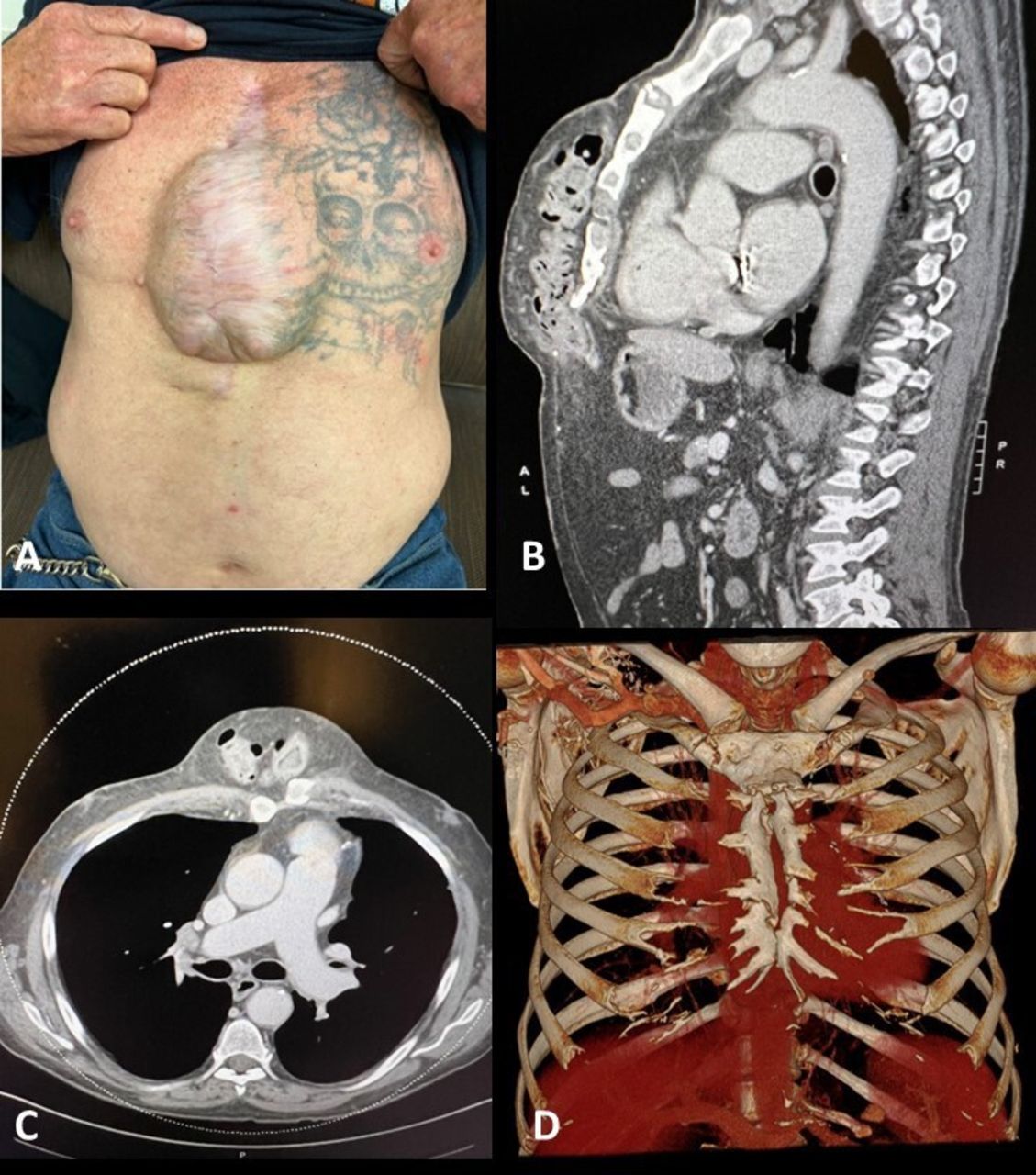
Initial presentation. (A) Physical examination showing bulge over the chest wall. (B) Sagittal CT showing subxiphoid hernia containing colon. (C) Axial CT. (D) CT reconstruction showing sternal non-union.
The patient’s medical history was also notable for coronary artery disease, chronic obstructive pulmonary disease (COPD), chronic kidney disease, hypertension, chronic opioid use, former methamphetamine use, housing instability and lack of social support. He had continued taking ticagrelor after his coronary artery bypass graft despite absence of an indication. After an outpatient consultation with surgery, he had managed to quit smoking 8 weeks ago.
What would you do?
Non-operative management due to the patient’s significant comorbidities
Medical optimization, then open repair with permanent mesh and sternal plating
Medical optimization, then robotic repair with permanent mesh
Medical optimization, then open repair with permanent and biological mesh
What we did and why
The patient was admitted for surgical optimization. Ticagrelor was discontinued, whereas a COPD and hypertensive medication regimen was initiated. Physical and occupational therapists worked with the patient for prehabilitation. Eight days later, he underwent open subxiphoid hernia repair.
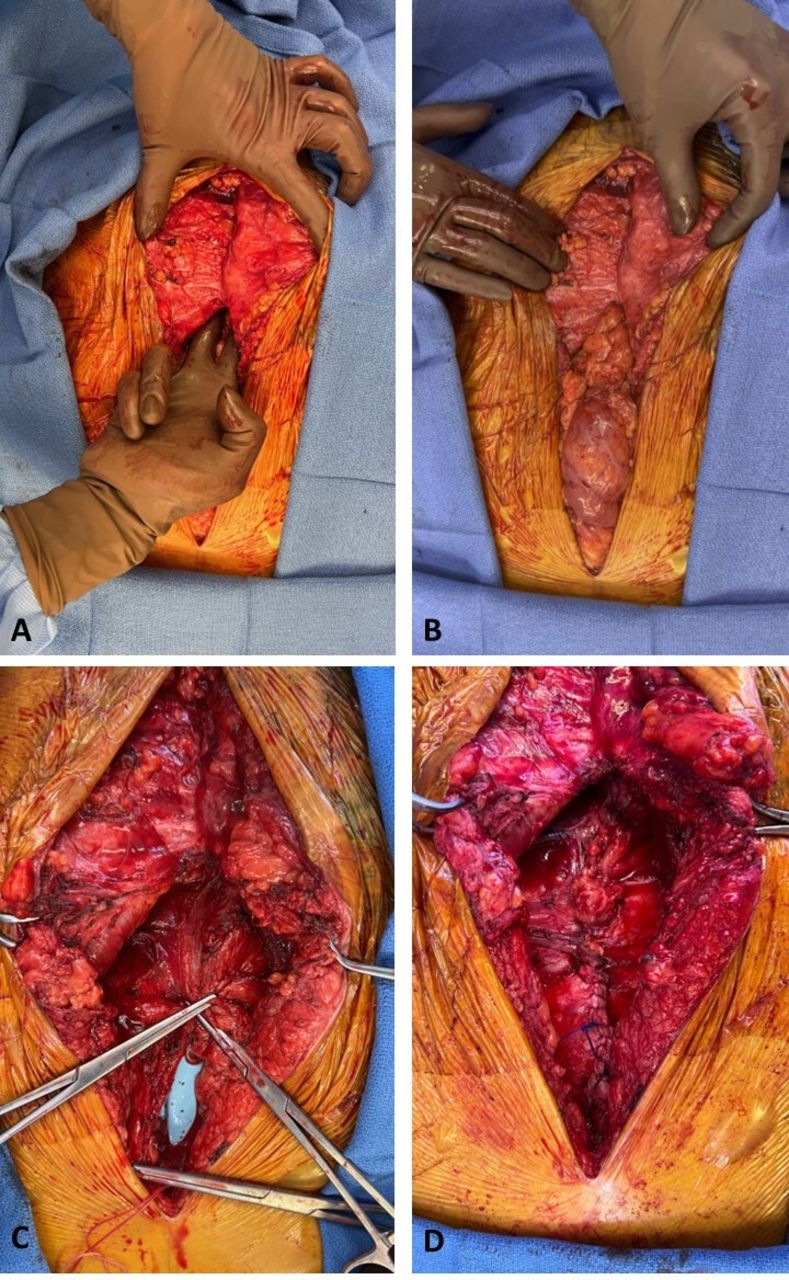
A midline sterno-abdominal incision was made from the supraumbilical abdomen extending upward over the hernia sac to the upper sternum. The peritoneal cavity was entered inferior to the hernia. Adhesions to the hernia sac were taken down, and colon was reduced into the abdomen. The upper aspect of the incision was fully opened, revealing a 2×8 cm fascial defect extending inferiorly from the xiphoid resection cavity. As the sternal non-union was overall stable on intraoperative manipulation, no sternal plating was performed (figure 2A,B).
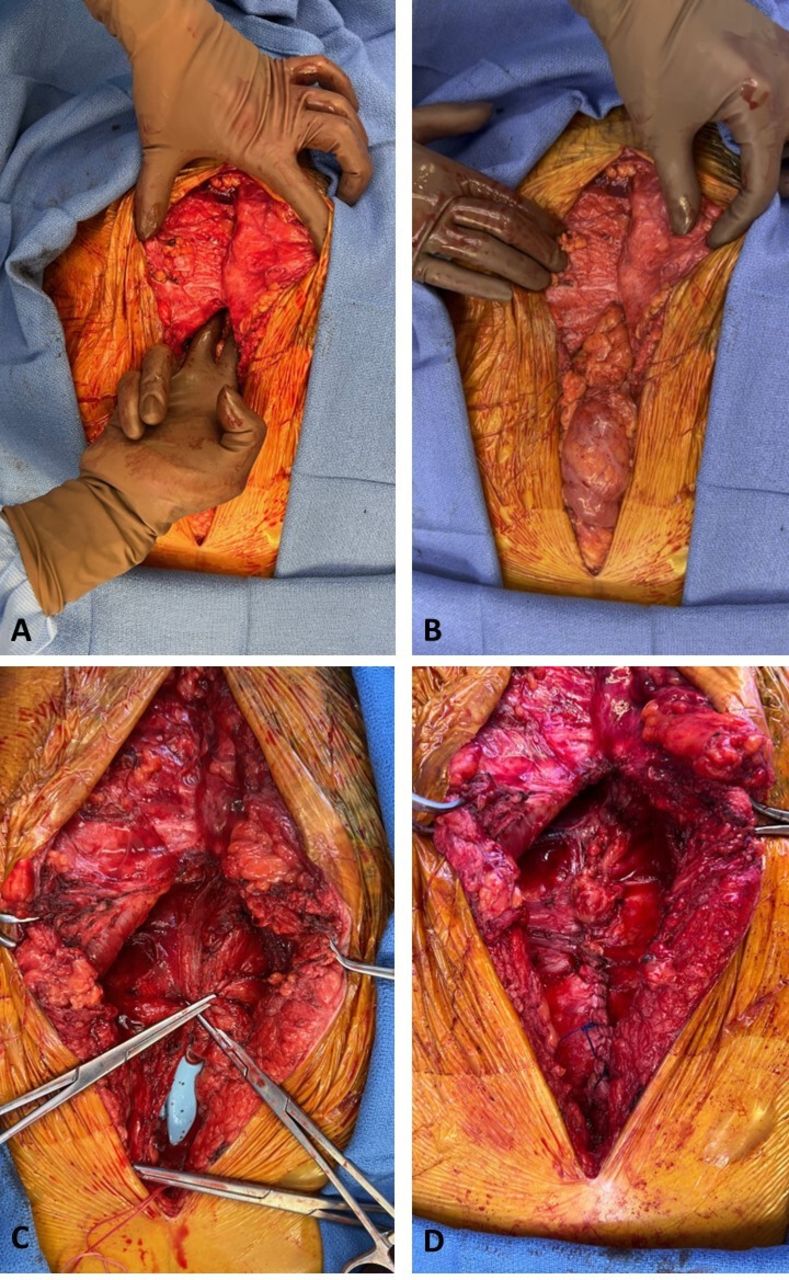
Exposure of defect. (A) Subxiphoid hernia defect. (B) Testing the sternum revealed no gross instability. (C) Retrorectus and retrosternal space freed up. (D) Posterior fascia closed primarily.
The rectus sheath was incised medially bilaterally, and the retrorectus plane was dissected. Superiorly, the substernal space was cleared by separating scarred pericardium and diaphragm from the undersurface of the sternum and chest wall up to 3 cm cephalad. Care was taken to avoid dissection of the patient’s cardiac vascular grafts. With all layers free, primary closure of the posterior sheath and scarred pericardium was obtained with running #1 prolene sutures and #1 vicryl retention sutures (figure 2C,D). A 20×30 cm Symbotex mesh was placed in the retrorectus and retrosternal space and anchored to the ribs and abdominal fascia with #1 prolene (figure 3A). There was at least 2 cm mesh overlap circumferentially. Two drains were placed. Once the anterior sheath was closed over the mesh, the defect from the previously resected xiphoid remained (figure 3B). To cover this defect and reinforce the repair, bilateral myocutaneous flaps were mobilized, and an onlay 40×20 cm Enform mesh was anchored to the anterior chest wall and anterior rectus sheath with absorbable tacks (figure 3C). The pectoralis major was detached from the sternum and reinserted above the mesh as a pectoralis major flap. Two more drains were placed. The skin and subcutaneous tissue were closed in layers (figure 3D), and a Prevena wound vacuum was applied. The patient recovered uneventfully and was discharged to a rehabilitation facility. Follow-up CT scans at 3 months have shown no recurrence.

{kind=link}
{kind=link}
{kind=link}
Completion of repair. (A) Symbotex mesh placed. (B) Anterior fascia closed over the mesh, with forceps inserted into residual sternal defect. (C) Enform onlay mesh tacked into place. (D) Closure.
Subxiphoid hernia is a rare complication that develops in 1.0% to 4.2% of patients after sternotomy, particularly after debridement of an infected sternal wound.1–3 Open and laparoscopic techniques have been described, each attempting to mitigate the high recurrence rate at this high-tension location (up to 80% recurrence without mesh4 or up to 32% with mesh5–7). Laparoscopic repair may have higher recurrence rates8 9; given the chronically incarcerated colon and the possibility of sternal plating, an open approach was chosen in this patient. To our knowledge, the mesh sandwich technique used for this patient has not been previously described for repair of subxiphoid hernias, though it has been used for hernias elsewhere.10 11 We thought it would be helpful given the size of the defect, chronically incarcerated colon, comorbidities of the patient and absent xiphoid process.
Ethics statements
Patient consent for publication
Footnotes
Contributors JPA wrote the article. JDF edited the article and supervised its writing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.