Article Text

Abstract
Objectives Chronic critical illness (CCI) is a phenotype that occurs frequently in patients with severe injury. Previous work has suggested that inflammatory changes leading to CCI occur early following injury. However, the modifiable factors associated with CCI are unknown. We hypothesized that hypothermia, an early modifiable factor, is associated with CCI.
Methods To determine the association of hypothermia and CCI, a secondary analysis of the Inflammation and Host Response to Injury database was performed, and subsequently validated on a similar cohort of patients from a single level 1 trauma center from January 2015 to December 2019. Hypothermia was defined as initial body temperature ≤34.5°C. CCI was defined as death or sustained multiorgan failure ≥14 days after injury. Data were analyzed using univariable analyses with Student’s t-test and Pearson’s χ2 test, and logistic regression. An arrayed genomic analysis of the transcriptome of circulating immune cells was performed in these patients.
Results Of the initial 1675 patients, 254 had hypothermia and 1421 did not. On univariable analysis, 120/254 (47.2%) of patients with hypothermia had CCI, compared with 520/1421 (36.6%) without hypothermia who had CCI, p<0.001. On multivariable logistic regression, hypothermia was independently associated with CCI, OR 1.61 (95% CI 1.17 to 2.21) but not mortality. Subsequent validation in 1264 patients of which 172 (13.6%) were hypothermic, verified that hypothermia was independently associated with CCI on multivariable logistic regression, OR 1.84 (95% CI 1.21 to 2.41). Transcriptomic analysis in hypothermic and non-hypothermic patients revealed unique cellular-specific genomic changes to only circulating monocytes, without any distinct effect on neutrophils or lymphocytes.
Conclusions Hypothermia is associated with the development of CCI in severely injured patients. There are transcriptomic changes which indicate that the changes induced by hypothermia may be associated with persistent CCI. Thus, early reversal of hypothermia following injury may prevent the CCI.
Level of evidence III.
- multiple trauma
- multiple organ failure
Data availability statement
Data are available in a public, open access repository. Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All previous data were able to be obtained on public open access website (gluegrant.org). However, data on this particular study are presented in the manuscript, and additional data can be provided on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Traumatic injury has been the leading cause of death in high-income countries for patients <45 years of age over the last 40 years.1 2 Fortunately, advances in prehospital care and the establishment of effective trauma systems have improved in-hospital mortality following traumatic injury.3 4 This has largely been achieved through early identification of injury and targeted management avoid the lethal triad of hypothermia, acidosis and coagulopathy.5 As initial injury management results in fewer early trauma deaths, the importance of understanding the factors that impact late trauma morbidity and mortality has increased.6
Improved early survival has been associated with an increase in the number of patients who have long intensive care unit (ICU) stays that is often associated with persistent organ dysfunction, a condition termed chronic critical illness (CCI).7 8 CCI has come to describe the prolonged ICU care and poor clinical outcome of a diverse spectrum of conditions, but a consensus definition has not emerged.9 10 Despite variations in the exact definition of CCI, its recognition as a distinct clinical entity has spurred a growing collection of studies precisely aimed at understanding which patients develop CCI and how best to manage it.10–13 Efforts to understand CCI physiology has demonstrated the importance of the immunological sequelae of trauma, organ failure and poor long-term outcome.4 8 14–16
Traumatic injury induces both the pro-inflammatory systemic inflammatory response syndrome and a compensatory anti-inflammatory response syndrome. Persistent dysregulation of the balance of these immune responses has been associated with CCI following severe trauma.14 Ongoing dysregulation of these pathways may be similar to the immune dysfunction observed in patients with poor outcomes following other causes of critical illness like sepsis, which leads to the development of persistent inflammatory catabolic syndrome (PICS).17–20 Infections in patients at risk are frequently responsible for late deaths weeks after injury, making a unifying mechanism of immunological dysfunction a compelling explanation.4 21–24 Some genomic changes associated with persistent organ dysfunction appear to occur soon after injury, even within the first few hours, which would offer an opportunity to identify and mitigate early immune dysfunction and potentially reduce the risk of CCI.4 14 21
There are similar knowledge gaps regarding the impact on immunological effects of hypothermia after severe injury. Hypothermia immediately following severe traumatic injury is associated with poor short-term and long-term outcomes.25–30 Recently, hypothermia has been associated with increased mortality in patients that are massively transfused requiring significantly more blood products than non-hypothermic patient.31 Although the effect of hypothermia maybe due to increased blood loss and blood product utilization, this recent study and several other studies suggest that hypothermia may be an independent factor that contributes to both early and late mortality.31–35 However, some degree of hypothermia is protective for conditions of ischemia/reperfusion, such as been demonstrated most commonly following cardiac arrest and during cardiopulmonary surgery.36 37 Thus, this raises the question of if and why hypothermia following injury may be associated with poor outcome and late mortality, compared with other ischemia/reperfusion conditions.
This study seeks to address this fundamental gap in understanding of the immunological effect of hypothermia, and sustained clinical immunological effects demonstrated as CCI and mortality. We hypothesize that admission hypothermia is associated with the development of CCI, and that this is driven by a dysregulated immunological response.
Materials and methods
Study design
To investigate this, we queried the Inflammation and the Host Response to Injury Program database (Trauma Glue Grant).38 In this observational, prospective study conducted from November 2003 to September 2013 at seven US level 1 trauma centers. Inclusion criteria were patients aged ≥18 years, confirmation of severe blunt traumatic injury with hemorrhagic shock (systolic blood pressure <90 mm Hg or base deficit (BD) of ≥6 mEq/L within 60 min of arrival) and required initiation of blood transfusion within 6 hours of arrival. Patients expected to survive <48 hours and those with severe traumatic brain injury (TBI; Glasgow Coma Scale <8 and abnormal head CT) were excluded. Study subjects were treated under the guidance of standard operating procedures developed, implemented and audited across all participating centers to minimize treatment variation as described previously. Demographic, clinical, physiological and outcomes data were obtained and studied for the first 28 days after injury, or until ICU discharge.
To assess the initial immunological and genomic response to severe blunt trauma and hypothermia, the genomics data of individual cell types present in the Trauma Glue Grant database was used. These data were initially collected using The Glue Grant Human Transcriptome Array (GG-H)—a comprehensively designed probe set which interrogates various aspects of the transcriptome predominantly in inflammatory cells (online supplemental table 1). Peripheral blood monocytes, neutrophils and lymphocytes were collected from 252 severe blunt trauma patients under the age of 55 years who consented to blood sampling. The first blood sample was taken within 12 hours of the injury and 1, 4, 7, 14, 21 and 28 days after injury and their genomic expression profile at each time point analyzed using GG-H chips. We excluded patients without a documented initial temperature and those with microarray data for only one time point and whose microarray RNA quality score was <2. Microarray data for the initial time point (blood draw occurring within 12 hours of injury) were downloaded from the TRDB website (http://www.gluegrant.org/) and then normalized using DNA Chip Analyzer 2007 software (dChip, freeware available at http://www.dchip.org/).
Supplemental material
Given change in resuscitation practices that were adopted after the completion of the Trauma Glue Grant database, a cohort of patients with identical inclusion criteria were reviewed from a single level 1 trauma center, Harborview Medical Center, from January 2015 to December 2019 to determine if the relationships between hypothermia and CCI was similar. Genomic data were not available for these patients.
Definition and outcomes
Among study subjects, admission hypothermia was defined as a trauma bay temperature of ≤34.5°C. The primary outcome variable was the incidence of CCI. Secondary outcomes included nosocomial infections, hospital length of stay and morality. Currently, there is no consensus definition for CCI. Given this ambiguity, we elected to define CCI as prolonged ICU admission (≥14 days) with evidence of ongoing organ dysfunction. This definition is based on the Trauma Glue Grant experience that patients meeting these criteria demonstrate a prolonged, dysregulated genomic response to injury, persistent organ dysfunction and adverse outcomes.39 We defined persistent organ dysfunction using the Modified Marshall’s Multiple Organ Dysfunction Score criteria, specifically excluding neurological component because of potential concurrent TBI, requiring either ≥2 in the renal (serum creatinine ≥1.9 mg/dL (without dialysis)) or pulmonary (Pao2/Fio2 ≤300) categories, or ≥1 in the cardiac category (systolic blood pressure <90 mm Hg, or use of vasopressors).7 8 14
Statistical analysis
For the initial cohort of patients, data are presented as means with SD for continuous variables compared using Student’s t-test, whereas those not satisfying normality were compared using the Kruskal-Wallis test. Categorical variables are presented as frequency and percentage and compared using the Pearson’s χ2 test or Fisher’s exact test. For multivariable logistic regression analysis, we a priori selected explanatory variables including age, sex, body mass index (BMI), injury severity score, initial international normalized ratio (INR) ≥1.5 and shock as defined as either initial lactate (>4) and/or initial BD (≤6). We also included treating center in the final model. We report adjusted ORs with 95% CIs. Area under the receiver operating curve values and Hosmer-Lemeshow goodness-of-fit test were used to assess model discrimination and fit. To determine the interaction between hypothermia, shock and coagulopathy, the regression fit of the model with and without three-way interaction was compared, and the marginal effect of each factor was evaluated.
For the validation cohort of patients, univariant analysis was performed. For multivariable logistic regression analysis, a similar a priori explanatory set of variables were obtained excluding site and also included variables that were found to have a p<0.1 on univariant analysis. Variables included in the final validation model included age, sex, BMI, injury severity score, initial INR >1.5, presence of shock and transfer status.
For the genomic analysis and following normalization of microarray data, BRB-ArrayTools software (developed by Drs Richard Simon and Amy Peng Lam, freeware available at http://linus.nci.nih.gov/BRB-ArrayTools.html) was used to perform significance analysis of microarray (SAM) comparison as well as prediction analysis of microarray (PAM) class prediction modeling between traumatically injured patients and 25 healthy volunteer subjects contained in the database. Subsequently, separate SAM and PAM analyses were performed to compare patients that were normothermic (temperature >34.5°C) versus hypothermic (temperature ≤34.5°C). Significance for SAM analysis was determined using a false discovery rate of <0.001 with 1000 permutations of the dataset, while significance for PAM analysis was determined using p<0.001.
Finally, serial individual patient microarrays were divided into seven time point groups, roughly corresponding to the following times postinjury: 12 hours, 1 day, 4 days, 7 days, 14 days, 21 days and 28 days. BRB-ArrayTools was then used to perform a time series analysis using an analysis of variance for mixed effects in which gene expression was considered as a factor of time and presence of hypothermia. Significance for the time series analysis was set at p<0.001. In the case of both the static and time series genomic analysis, probe sets that significantly differed were entered into Ingenuity Pathways Analysis V.6 (Ingenuity Systems, Redwood, California, USA) for assessment of gene ontology and functionality (not reported here).
Results
We identified a cohort of 1675 blunt-injured patients in the Trauma Glue Grant database whose clinical data include emergency room (ER) temperature measurements. Of these, 254 (15.2%) were hypothermic. Patients with and without hypothermia did not significantly differ in age, sex or BMI, but they did have significantly higher Injury Severity Score (ISS) and coagulopathy (table 1). Additionally, patients with hypothermia were more likely to be in shock with elevated lactate and BD. On univariable analysis, of the 1421 patients with normothermia on admission, 520 (35.6%) went on to develop CCI while 122 (48%) in the hypothermia group went on to develop CCI (p<0.001) (table 2). Moreover, univariable analysis revealed a significant association of hypothermia on CCI (p=0.001) and mortality (p=0.003) but no significant association on nosocomial infection or pneumonia (figure 1). Hypothermia on admission was also associated with significantly higher mean transfusion of red blood cells, fresh frozen plasma and platelets (table 2).
Patient characteristics with and without hypothermia on admission
Patientoutcomes with and without hypothermia on admission
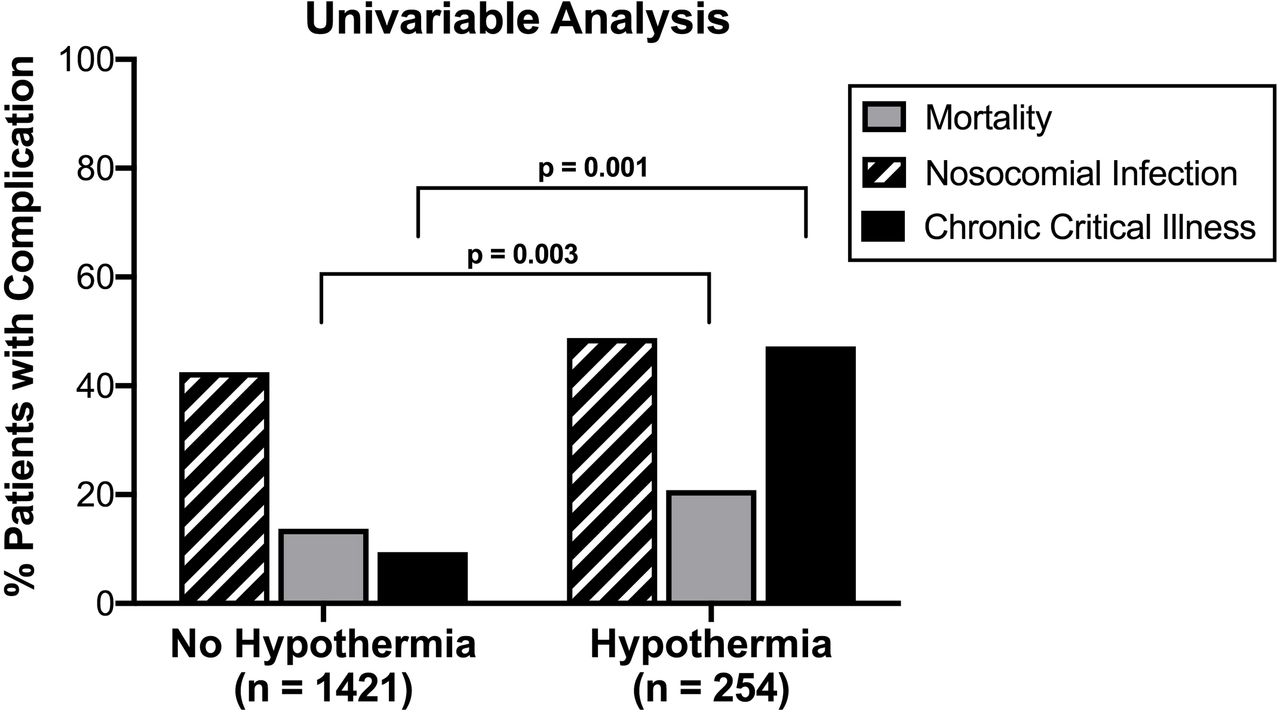
Clinical outcomes based on admission hypothermia.
Multivariable logistic regression to assess the effect of various admission factors on CCI including mortality revealed a significant association with age (OR 1.03 (95% CI 1.02 to 1.04), p<0.001), BMI (OR 1.05 (95% CI 1.03 to 1.07), p<0.001), shock (OR 1.37 (95% CI 1.07 to 1.76), p=0.013), INR ≥1.5 (OR 1.94 (95% CI 1.48 to 2.56), p<0.001) and ISS (OR 1.06 (95% CI 1.05 to 1.07), p<0.001) on the development of CCI. Hypothermia was associated with CCI when controlling for all other variables (OR 1.61 (95% CI 1.17 to 2.21), p=0.004) (table 3). Treatment at site 8 and coagulopathy were also significantly associated with CCI. Patients treated at site 3 had lowers odds of developing CCI. Treatment at any of the other sites was not significantly associated with CCI. Evaluation of the goodness of fit of the model demonstrated a good fit of the model, with an area under the curve of 0.75 and Hosmer-Lemeshow test with a p value of 0.75. Hypothermia was not associated with mortality (OR 1.48 (95% CI 1 to 2.2), p=0.052) or nosocomial infection (OR 1.1 (95% CI 0.841.51), p=0.431) on multivariable analysis.
Multivariable analysis of impact of hypothermia on CCI
Because hypothermia, shock and coagulopathy interact, we evaluated the effect of including three-way interaction terms of the fit of the model (online supplemental table 1), the likelihood ratio (LR) test demonstrated that interaction terms did not significantly improve the fit of the model (p=0.71), and none of the interaction terms were significant (shock and hypothermia: p=0.39, hypothermia and coagulopathy: p=0.44, coagulopathy and shock: p=0.25 and all three: p=0.46). Finally, we assessed the marginal contribution of each factor to the result of CCI with all other variables set to the mean. An otherwise average patient in the dataset without hypothermia, shock or coagulopathy had a 0.29 (95% CI 0.25 to 0.33) probability of developing CCI. An average patient with only hypothermia had probability of 0.38 (95% CI 0.22 to 0.54), while those with only shock had a probability of 0.33 (95% CI 0.3 to 0.37) and those with only coagulopathy had a probability of 0.39 (95% CI 0.3 to 0.49). An average patient with all three had a probability of 0.58 (95% CI 0.5 to 0.67). Thus, it appears that the interactions between the three variables are minimal so, to improve interpretability of the model, we omitted the interaction terms in the regression model.
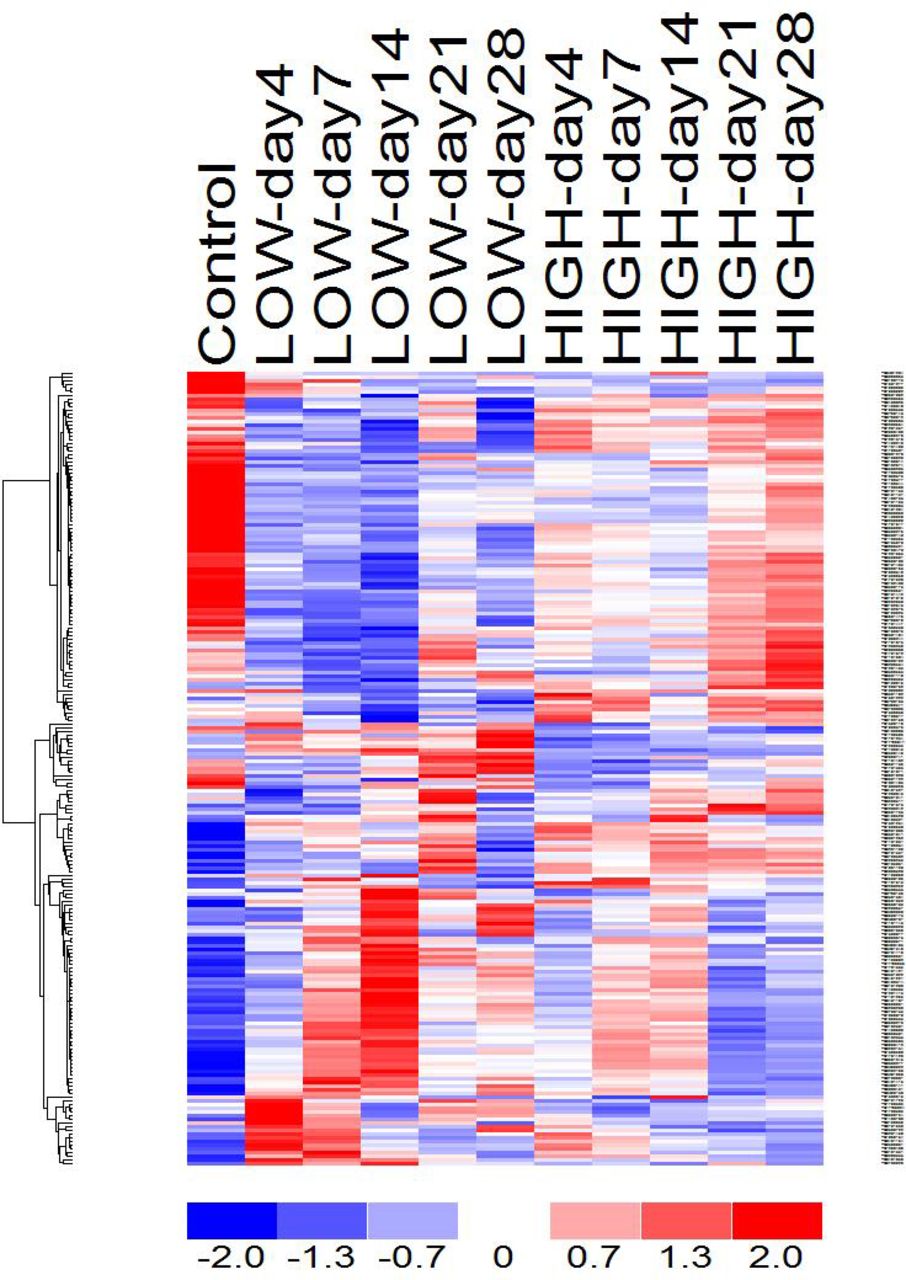
Given this clinically apparent immunological effect, we evaluated the genomic transcriptome of a subset of patients included in the outcome regression analysis. Microarray analysis of a broad set of monocyte RNA transcripts were retrospectively analyzed for patterns of fold change associated with hypothermia (online supplemental table 2). There was no significant signal of either upregulation or downregulation in transcription among this probeset in circulating neutrophils or lymphocytes between the hypothermia and non-hypothermia subjects. However, unsupervised analysis of monocyte transcripts did reveal a marked durable genomic dysregulation of over 100 transcripts persistent at 4 weeks postinjury compared with control and non-hypothermic patients (figure 2). Notably, at day 4 in the hypothermic cohort, sustained upregulation of pro-inflammatory cytokines was evident with persistent alterations in tumour necrosis factor-α and interferon-γ. Importantly, components of antigen presentation including major histocompatibility complex (MHC) II was downregulated at day 4. Although the overall degree of dysregulation did diminish over time, alterations in antigen presentation persisted throughout the first day 28 of the study.
{kind=link}
{kind=link}
Unsupervised RNA array of circulating monocytes.
Finally, given changes in resuscitation and clinical practice over time, the findings of the initial multicenter cohort of patients with associated genomic data were validated on set of patients meeting the same initial study inclusion criteria from January 2015 to December 2019 from a single level 1 trauma center, Harborview Medical Center. One thousand two hundred sixty-four blunt-injured patients were identified, of which 172 (13.6%) presented with hypothermia. Similar to the initial cohort, patients with and without hypothermia did not significantly differ in age, sex or BMI, but they did have significantly higher ISS, blood product transfusions, coagulopathy and presented in more severe shock. On univariable analysis, of the 1092 patients with normothermia on admission, 284 (%) went on to develop CCI while 68 (39.5%) in the hypothermia group went on to develop CCI (p<0.001). Multivariable logistic regression including the various admission factors described demonstrated that age, ISS, red blood cell (RBC) transfusion, shock and hypothermia remained independent predictors of CCI, and transfer status to remain independently associate with CCI (table 4). Hypothermia in this cohort was not associated with mortality.
Multivariable analysis of impact of hypothermia on CCI in recent validation cohort
Discussion
In this study, we demonstrate that hypothermia in severely blunt injured patients is associated with development of CCI but not associated with increased risk of death which recapitulates earlier work on this subject.26 Our early transcriptional analysis also found a significant, broad downregulation in several gene pathways from circulating monocytes, but not lymphocytes or neutrophils, in hypothermic patients compared with normothermic patients. This is a critical and novel finding demonstrating specific cellular effects of hypothermia. Mixed-cell population analysis did not demonstrate this downregulation, which only became significant in granular analysis of specific cell lines. These data indicate hypothermia may be a major driver of CCI by way of dysregulating immune function early and sustained for several weeks following initial injury. Importantly, the sustained downregulation in the ability for monocytes to present antigen may result in late infectious complications, in addition to the independent association of the genomic changes induced by hypothermia.
The changing epidemiology of trauma morbidity and mortality warrants investigation about the nature of late adverse outcomes. The patients who benefit from improved early mortality are now surviving their initial trauma only to die many weeks later.4 21 23 24 40 It follows that there may be lasting alterations in these patients’ physiology, and PICS is an emerging phenotype which may underlie this phenomenon. This study demonstrated a clear association between hypothermia and the clinical entity of CCI, which appears to be associated with ongoing organ failure or death even when controlling for other markers of severe injury early in trauma, including shock, coagulopathy and blood transfusion.
Hypothermia in severely injured patients is closely linked to other drivers of mortality and long-term morbidity, including shock and coagulopathy, making analysis of the impact of each individual factor on CCI more difficult. However, when correcting for shock and coagulopathy, hypothermia remained an independent factor associated with the development of CCI in both cohort of patients. Furthermore, we evaluated the interaction of these three terms together and did not find their interaction greatly influenced by the results of our model. Importantly, although continued improvement in resuscitation and clinical care continued, the most recent cohort supports this unique finding of hypothermia altering inflammation and being associated with CCI. Together, these clinical data support the novel genomic data showing significant changes selectively within monocytes early on following severe injury and hypothermia. Because of the confounding direct effect of hypothermia and transfusion, an additional regression analysis was performed that included an interaction between RBC transfusions. This analysis supported hypothermia being independently associated with CCI despite the potential contribution of blood transfusion. Interestingly, hypothermia was not independently associated with mortality. This finding is intriguing and suggests the CCI associated with hypothermia is driven by sustained organ dysfunction and not death. Thus, the direct effects on inflammation and sustained inflammatory alterations demonstrated in the genomic analysis suggests a potential role of hypothermia on sustained organ dysfunction.
The findings of this study are important because the initial inflammatory genomic dataset is the largest cohort to date that contains linked clinical data to multiple time-point transcriptomic data. Demonstrating and validating the initial and sustained inflammatory contribution to hypothermia, and development of sustained inflammatory clinical dysfunction in CCI is important in determining potential long-term effects of a relatively frequent clinical event in hypothermia. Although CCI is likely multifactorial in nature, it appears that hypothermia may be a critical and potentially modifiable factor involved. Our analysis when controlling for several key covariants demonstrated a strong association between hypothermia, immune dysregulation and CCI.
The overall immunological response to trauma is remarkably complex and remains poorly understood. The changes in inflammatory mediators, antigen presentation, T cell proliferation and function and natural killer cell function seen following trauma are similar to changes seen following low-dose bacterial endotoxin injection and appear to begin at the time of injury.14 41 This is consistent with a hypothesis of non-resolving inflammation, but immunosuppression is also present following sepsis and trauma indicating these states actually lead to a mixed inflammatory picture.42 43 Because this study demonstrated immunological changes early following injury, there is a plausible role for hypothermia in these alterations. The changes, however, are specific and only occurred in circulating monocytes without changes in neutrophils or lymphocytes. This finding provides evidence that the immune response to trauma likely represents a fundamental, initial genomic response to severe inflammation and the acute onset of a chronic inflammatory phenotype that is affected by the initial clinical state. The early transcriptomic response in these hypothermic patients clearly shows a gross global dysregulation in inflammatory genes that appears to wane gradually with time but that persists up to 4 weeks and potentially longer after injury. Among the initial changes is an upregulation of pro-inflammatory cytokines that is associated with a concurrent downregulation of antigen presentation, in particular of MHC II genes. This immune dysregulation may result in persistent immune dysfunction, PICS, severe infections and late death following discharge.7 44 The available data currently hint that these changes start quite early after injury, and thus the opportunity to intervene on CCI by correcting hypothermia may improve outcomes.45 This emphasizes the need to better understand the relative importance of hypothermia on genomic expression in immune regulation and the association with clinical outcome and long-term complications.
There are a number of key limitations to this study which contextualize these findings and clarify how to optimally apply the results. While these data were analyzed retrospectively, the initial cohort of data was prospectively collected from the largest multicenter trauma database that includes admission vital signs and matched blood samples making it the optimal available study population for long-term physiological and inflammatory effects of hypothermia. Nevertheless, the study was not designed to collect enough blood samples at predetermined intervals on enough hypothermic patients to make causal conclusions beyond the associations described here. Additionally, although variations in clinical practice could potentially affect these results, the effects of changes in resuscitation practice and recent clinical care were supported by the recent validation cohort. Furthemore, the temperature of 34.5°C was used as the cut-off for admission hypothermia as it is a common cut-off in clinical trauma papers despite being warmer than 32°C, which is the temperature that animal studies suggest is associated with a significant impairment in clotting function.46 47 Still, both of these cohorts represent a large, pragmatic, heterogeneous trauma population that is broadly sampled and contains clinically meaningful physiology markers. Regarding the utility of studying admission hypothermia as a modifiable risk factor, it is true that correcting body temperature prior to arrival in the ED can be challenging; however, early intervention on hypothermia does represent a target for intervention. It is interesting that transfer status in the validation cohort and thus sustained hypothermia was independently associated with CCI, but the role of rewarming and duration of shock was not able to be separated within this specific cohort. Our future work focuses on rewarming techniques, rate of rewarming and their effect on CCI.
With respect to the genetic analysis, we analyzed the transcriptomic response of circulating monocytes, neutrophils and lymphocytes, but compartmentalization of the inflammatory response is a well-known phenomenon. Importantly, while we were not able to clearly see recapitulated transcriptomic changes in neutrophils or leukocytes, we did uncover a detailed and likely important cell-line-specific transcriptome change. We were unable to investigate the transcriptome of these cells in secondary lymphoid organs and the reticuloendothelial system which would have allowed more granular topography about the time and location of transcriptomic changes. Additionally, as patients convalesced, the sampling intervals became longer, potentially missing brief secondary immunological responses. Finally, as other parts of clinical practice evolve including resuscitation and critical care, the isolated effect of hypothermia may be altered. Thus, this study similar to the retrospective nature of this analysis is subject to potential current and future changes in practice. However, the specific contribution of hypothermia remains important.
The past 50 years of trauma care has been marked by continuous improvement in prehospital, operative and ICU care targeted at managing the lethal triad of acidosis, coagulopathy and hypothermia.5 Patients who survive longer after their initial trauma are at risk for long-term physiological changes and disability. As our ability to keep patients alive through their acute resuscitation improves, identifying and correcting risk factors for poor long-term outcomes is increasingly imperative. Admission hypothermia does appear to be independently associated with CCI following traumatic injury, and this work illuminates immune dysregulation as a possible mechanism for this delayed clinical syndrome. Significant future investigation will shed light on the important impacts of rapid correction of hypothermia on the host immune response and delayed outcomes.
Data availability statement
Data are available in a public, open access repository. Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All previous data were able to be obtained on public open access website (gluegrant.org). However, data on this particular study are presented in the manuscript, and additional data can be provided on request.
Ethics statements
Ethics approval
IRB Study 00013012.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators none.
Contributors All authors contributed to the analysis, writing and critical revisions of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.