Article Text

Abstract
Background Trauma systems in rural areas often require longdistance transfers for definitive care. Delays in care, such as delayed femurfracture repair have been reported to be associated with poorer outcomes, butlittle is known about how transfer time affects time to repair or outcomesafter femur fractures.
Methods We conducted a retrospective review of all trauma patients transferred to our level 1 rural trauma center between May 1, 2016-April 30, 2019. Patient demographics and outcomes were abstracted from chart and trauma registry review. All patients with femur fractures were identified. Transfer time was defined as the time from admission at the initial hospital to admission at the trauma center, and time to repair was defined as time from admission to the trauma center until operative start time. Our outcome variables were mortality, in-hospital complications, and hospital length of stay (LOS).
Results Over the study period1,887 patients were transferred to our level 1 trauma center and 398 had afemur fracture. Compared to the entire transfer cohort, femur fracture patientswere older (71 versus 57 years), and more likely to be female (62% versus 43%).The majority (74%) of patients underwent fracture repair within 24hours. Delay in fracture fixation >24 hours wasassociated with increased length of stay (5 days versus 4 days; p<0.001),higher complication rates (23% versus 12%; p=0.01), and decreased dischargehome (19% vs. 32%, pp=0.02), but was not associated with mortality (6% versus5%; p=0.75). Transfer time and time at the initial hospital were not associatedwith mortality, complication rate, or time to femur fixation.
Discussion Fixation delay greater than 24 hours associated with increased likelihood of in-hospital complications, longer length of stay, and decreased likelihood of dischargehome. Transfer time not related to patient outcomes or time to femur fixation.
Level of evidence Level III; therapeutic/care management.
- femoral fractures
- outcome assessment
- health care
- time-to-treatment
Data availability statement
Data are available upon reasonable request. Data are available as deidentified participant data upon request. Please contact the corresponding author at kristin.colling@essentiahealth.org.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In traumatic injury, time to treatment matters. As in other aspects of medical care, rapid treatment in trauma resuscitation is associated with better outcomes, just as time to TPA receipt in ischemic stroke1 and time to catheterization in myocardial infarctions lead to better outcomes.2 When compared with urban patients, rural patients have significantly increased odds of death from traumatic injury, likely due at least in part to delays in treatment.3–5 Rural patients are often first evaluated at a local critical access hospital and subsequently transferred to a trauma center for definitive care. When appropriately and expediently transferred, transfer patients seem to do as well as patients admitted directly to the trauma center6; however, delayed transfers or failure to transfer is associated with decreased survival.7 Recently, improved patient outcomes and decreased length of stay have been associated with femur fracture repair within 24 hours of admission.8 9 For patients who require transfer to a trauma center, especially rural patients who may require long-distance transfer for repair, it is not known how the increased time from injury, including transfer time and time to fixation, relates to patient outcomes. Therefore, in this study, we evaluated the effects of transfer time on time to femur fracture repair and patient outcomes.
Methods
We performed a retrospective review of all consecutive patients transferred to our American College of Surgeons (ACS)-verified trauma center located in northeastern Minnesota between May 1, 2016 and April 30, 2019. Prior to October 2018, the trauma center was a level 2 ACS adult trauma center, and in October 2018 received level 1 verification. Patients were included if they met the National Trauma Data Standard patient inclusion criteria.10 Our study cohort was defined as all transfer patients admitted with either a femoral neck, intertrochanteric, femoral shaft, or distal femur fracture who underwent surgical intervention at our hospital. Any patients who elected not to participate in research, did not have a femur fracture, or elected for non-operative management were excluded from the study. Patients who had a planned repair but died prior to the operation were included in the study (only one patient met this criterion).
Patient demographics, including age, sex, race, and primary residential locality (rural vs. urban as defined by Rural-Urban Area Community Codes11), were obtained from chart review and trauma registry, as were patients’ mechanism of injury, associated alcohol use, Injury Severity Score (ISS), hospital length of stay, mortality, and discharge disposition. In-hospital complications were noted as defined by the National Trauma Database.10 Elixhauser comorbidity scores were obtained for all patients. For patients transferred to our hospital, the mode of transportation (ambulance or helicopter) was recorded. Time spent at the initial hospital was defined as time from admission to time to discharge onto an ambulance or helicopter. Transportation time was defined as time from discharge from the initial hospital until time of admission to the trauma center. Total transfer time is defined as the total time from admission to the initial local hospital until time of admission to our trauma center. Time to repair of the femur fracture was calculated from the time of admission to our trauma center until operating room admission. In our main cohort, all patients with a femur fracture were evaluated for time to fixation and outcomes. Subgroup analysis of geriatric patients, who may be at greatest risk for delayed fixation, was performed.
This study was reviewed by the Essentia Institute of Rural Health Research Protection Program and was determined to not meet the definition of research with human subjects based on the guidance from the Office for Human Research Protections12 as this was a quality improvement project. As such, this study did not require or receive review by our full institutional review board.
Data analysis
All data were analyzed using IBM SPSS Statistics V.26. Statistics were performed using Mann-Whitney U test for all non-parametric variables and Student’s t-tests for all normally distributed variables. Categorical variables were analyzed using Pearson’s χ2 or, where cell frequency count was less than 5, Fisher’s exact test. For all analyses, p<0.05 was considered statistically significant. Binary logistic regression was used to analyze continuous variables’ effect on binary outcomes. A heat map of patients’ home location was created with ArcGIS V.10.8 (ESRI, ArcGIS Online, computer software; released February 2020; Environmental Systems Research Institute, Redlands, CA; retrieved https://www.arcgis.com/home/index.html) using patient zip codes.
Results
Between May 1, 2016 and April 30, 2019, 1837 trauma patients were transferred to Saint Mary’s Medical Center and were admitted. Over half of the patients were male (57.3%) and majority were Caucasian (table 1). The mean age was 56.9 years (Standard deviation (SD) 24.6). The median ISS was 9 (Interquartile Range (IQR) 5–9) and most patients were injured via blunt mechanism. Alcohol was associated with the injury in 16% of patients. The in-hospital mortality rate for all trauma patients was 1.7%.
Descriptive statistics for all trauma transfers during the study period and the femur fracture subgroup
Three hundred and ninety-eight femur fracture patients who met the inclusion criteria were identified. Patients with femur fractures were more often female (62%) and the mean age was older than the overall trauma cohort (table 1). Most patients in both groups were transferred from rural hospitals and transfers were received from a wide service area (figure 1). The median ISS was 9. Alcohol was present at the time of injury for 36% of patients with femur fractures, compared with 16% in the entire transfer cohort. The in-hospital mortality rate was 1.8% and the 30-day mortality rate was 5.5%.

{kind=link}
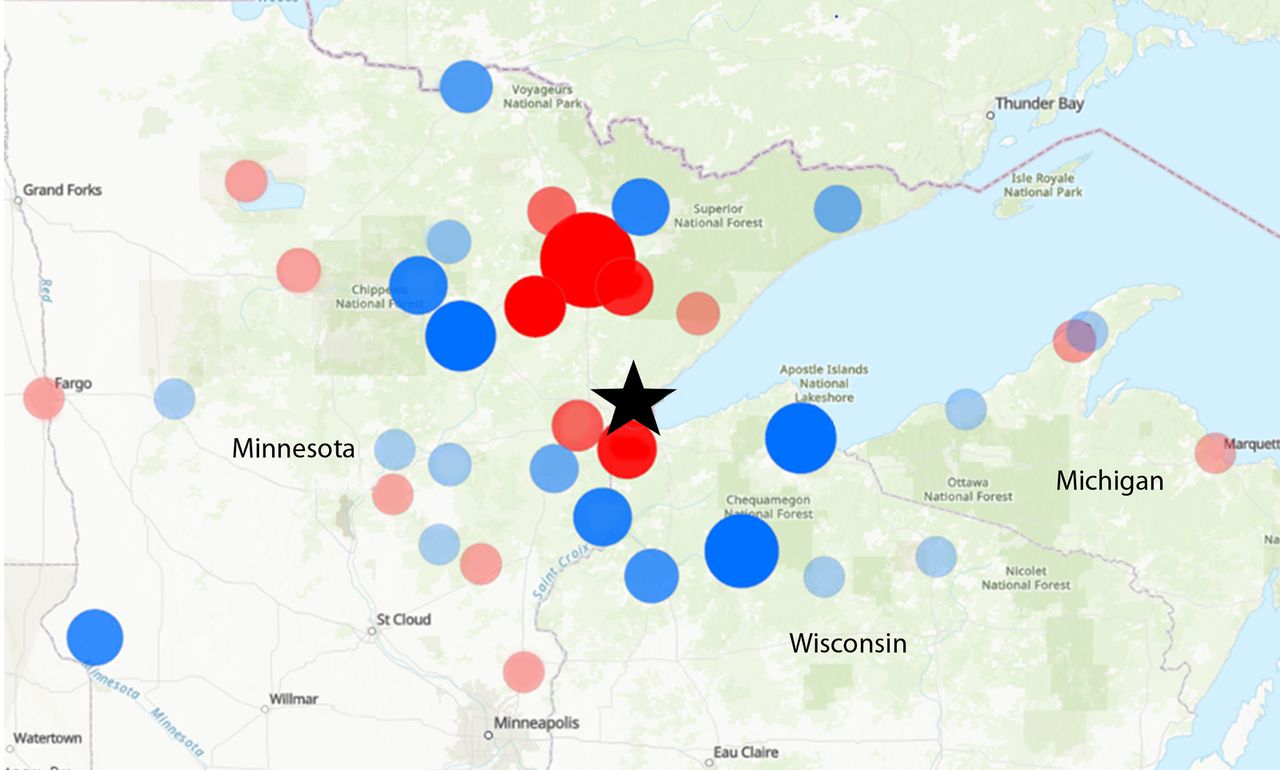
Heat map identifying locations of initial hospitals transfer patients with femur fractures to Saint Mary’s Medical Center (black star). Hospitals located in rural localities are in light gray, and urban/suburban hospitals are in black. The size of the circles corresponds to the relative number of patients transferred. The coverage area of our trauma system is quite large, spanning three states (Minnesota, Wisconsin, and Michigan) and serves a large rural population.
The median time spent at the initial hospital was 2.9 hours (IQR 2.3–4.1) and the median transportation time between hospital admissions was 1.48 hours (IQR 1.3–1.8). The median total transfer time was 4.5 hours (IQR 3.7–5.9). Most patients (82%) were from rural communities. Initial evaluation occurred at a level 4 ACS-designated trauma center in 67% of patients, 18% were evaluated at a level 3 ACS-designated trauma center, and 15% were evaluated at an undesignated trauma center. Ambulance transportation was used for the vast majority of patients (98%). Patients transferred by helicopter were significantly younger (median age 32 (IQR 11–57), p<0.0001), with higher ISS (median 10 (IQR 9–21), p=0.001) and had shorter transportation time (median 0.62 hours (IQR 0.6–0.8), p<0.0001). The median time to fracture fixation after presentation to the trauma center was 16.6 hours (IQR 11.0–24.3). Most patients (n=296, 74%) underwent fracture fixation within 24 hours of admission to the trauma center. There were no patient variables that were significantly associated with delayed fixation (table 2). There was no difference in patients’ age, sex, race, ISS, referring hospital trauma designation, or transfer times. However, patients who were admitted to the medicine service did have almost twice the rates of delayed fixation compared with patients admitted to the orthopedic trauma service or the trauma surgery service (47% compared with 23% admitted to orthopedic and 27% admitted to trauma service; p=0.009). Patients who were admitted primarily to the trauma service were significantly more injured (90% had ISS >15). Patients admitted primarily to the medicine service had a non-significant trend toward higher mean Elixhauser comorbidity scores (1.9 (SD 2.1) for medicine, compared with 1.3 (SD 1.7) and 0.7 (SD 1.5) for orthopedic and trauma surgery, respectively; p=0.06). All patients admitted to the medicine service had at least one chronic organ failure (most commonly cirrhosis and heart failure). On review of all patients admitted to medicine service who had a delay in fixation or greater than 24 hours, the most common reason for delay was “optimization” of a chronic condition (14 of 16 patients). Further cardiac testing, such as echocardiogram and stress tests, was performed in six patients, but no identified changes were made after obtaining these tests. Seven patients were delayed for optimization of cirrhosis or concerns for alcohol withdrawal. One patient was delayed due to orthopedic surgeon delaying the case until the next morning.
Patient demographic and injury data for patients with femur fractures, comparing those who underwent fixation within 24 hours of admission to trauma center and those repaired more than 24 hours from admission
Patients who had fixation greater than 24 hours from trauma center admission had significantly longer hospital length of stay, significantly less likely to be discharged home (19% vs. 32%, p=0.02, Relative Risk (RR) 0.49, 95% Confidence Interval (95% CI) 0.28 to 0.86), and were significantly more likely to have a complication (23% vs. 12%, p=0.01, RR 2.1, 95% CI 1.2 to 3.8). There was a trend toward greater need for intensive care unit stay, but this did not reach significance (10% vs. 5%, p=0.08). There was no difference in mortality rates for fixation within or after 24 hours.
Total transfer time and time at the initial hospital had no correlation with time to fracture fixation (Pearson’s correlation coefficient (PCC) 0.07, p=0.2). There was no correlation between total transfer time and hospital length of stay. There was a weak positive correlation between transfer time and age (PCC 0.126, p=0.01) and a weak negative correlation between transfer time and ISS (PCC −0.11). There was no significant difference in total transfer time (median 4.7 hours (IQR 3.8–6.8) compared with 4.5 hours (IQR 3.7–5.9); p=0.94) or time at initial hospital (median 3.1 hours (IQR 1.8–5.2) compared with 2.9 hours (IQR 2.3–4.1); p=0.97) between patients who died and who survived, respectively. There was no significant difference in transfer time or time at initial hospital between patients who did and did not have complications (table 3). Time to fracture fixation did positively correlate with patient age (PCC 0.153, p=0.002) and hospital length of stay (PCC 0.306, p<0.001). Using binary logistic regression for univariate analysis, the continuous variable of time to femur fixation, every hour of delay was significantly associated with increased risk of in-hospital complications (Odds Ratio (OR) 1.01, 95% CI 1.001 to 1.022), in-hospital mortality (OR 1.017, 95% CI 1.003 to 1.03), and decreased likelihood of being discharged home (OR 0.98, 95% CI 0.97 to 0.99).
Univariate analysis comparing patient variables and complication rates
Fifteen percent of patients (59 patients) had a complication in the hospital. In univariate analysis, complications were significantly associated with older age and longer time to fracture fixation (table 3). Sex, race, transfer time, or time at the initial hospital were not significantly associated with complications in univariate analysis. Multivariate regression was performed to assess the adjusted OR of fixation of fracture greater than 24 hours after admission on risk of complication when controlling for age, sex, and transfer time (table 4). Age and fracture fixation greater than 24 hours were independently associated with significantly increased risk of complication. Sex and transfer time were not associated with increased risk of complications in multivariate analysis.
Multivariate analysis for risk of complication after femur fracture repair using binary logistic regression
In subgroup analysis, evaluating only those patients 65 years of age and older, a total of 298 patients were identified. The median age was 81 (range 65–104). The median ISS was 9 (IQR 9–9). Compared with younger patients, this older cohort was more likely to be female (66% vs. 49%, p=0.002) and had a trend toward higher rates of Caucasian race (96% vs. 90%, p=0.06). Compared with patients younger than 65, this older cohort had longer median initial hospital stays (3.0 hours (IQR 2.4–4.3) vs. 2.6 hours (IQR 2–3.7), p=0.004), had longer median total transfer time (4.6 hours (IQR 3.9–6.0) vs. 4.0 hours (IQR 3.3–5.6), p=0.002), and had longer median time to fixation (17.7 hours (IQR 12.6–25.7) vs. 14.9 (IQR 6.8–20.8), p=0.001).
Fixation occurred within 24 hours of admission in 73% of the older patients. Delayed fixation in this subgroup was not associated with age, ISS, transport time, or time at the initial hospital. Hospital length of stay was significantly longer in patients with fixation delays greater than 24 hours (6 days (IQR 5–7.25) compared with 4 days (IQR 4–6); p<0.001). There was no difference in mortality between those patients who underwent fixation within 24 hours and those who did not (in-hospital: 2.8% compared with 1.2%; and 30-day mortality: 4.6% vs. 4.9%, respectively). Complication rate overall for those 65 and older was 17% and higher in patients who had delayed fixation (24% compared with 14%; p=0.05). Complication rate was not associated with initial hospital time prior to transfer or total transfer time. When only the younger age (less than 65 years) group (n=100) was evaluated, although not reaching statistical significance, patients with delayed fixation had a trend toward increased complication rates (15% compared with 5%; p=0.1) and was associated with significantly longer hospital stays (5 days (IQR 4–9.5) vs. 3 days (IQR 2–5), p<0.001).
Discussion
In this study, we found that although majority of patients underwent fixation of their femur fracture within 24 hours of admission to our trauma center, delay in femur fracture fixation greater than 24 hours was still associated with prolonged hospital length of stay, increased complication rates, and decreased likelihood of being discharged home. Although we did not find a significant increase in mortality with delay in fixation >24 hours, we did find that patients who died have a significantly longer median time to femur fixation.
This is the first study that we are aware of to evaluate transfer patient with femur fractures, enabling us to evaluate two separate time periods that could affect patient outcomes: time to fixation and time until admission to the trauma center. As our trauma center serves a large rural population, spanning three states (figure 1), we not only have a large catchment area, but also relatively long transportation times (median time after leaving the initial hospital to admission to our trauma center, ie, the drive time, was).
We did not find an association with transfer time and patient outcomes. There was also no correlation between transfer time and time to fixation. We did not find any other studies that evaluated the relationship between transfer times, times to repair of surgery, and outcomes in femur fracture patients. In our study, we did have relatively prompt transfer times to our trauma center after identifying the need for surgical intervention, which may have led to the lack of effect on patient outcomes. It is possible that in systems with less developed transfer patterns, transfer time could affect patient outcomes. Especially in rural trauma systems, where a large number of patients come from outlying and critical access hospitals, prompt transfer when needed is important, as delays in care can lead to worse outcome.13 Transfer times vary greatly throughout rural America, and all efforts should be made to expedite care.
Numerous other studies have evaluated time to femur fracture repair in recent years and have noted that delays in fracture repair have similar associations with poor patient outcomes,8 9 14 mortality,8 15 16 and increased hospital length of stay,8 14 as our study has found. Our rate of fracture fixation (74%) within 24 hours of admission to the trauma center was higher than most other studies, who have reported ranges of between 21% and 34% of patients having fracture repair within 24 hours.8 9 14 16 The optimum time to fixation is still unclear. The most recent meta-analysis performed by Klestil et al15 identified 28 prospective studies that evaluated time to femur fixation and outcome. This group found that femur fixation after 48 hours was associated with a 20% lower risk of dying within 12 months (RR 0.80, 95% CI 0.66 to 0.97), but concluded that fixation within 24 hours was not significantly associated with lower risk of mortality, although RR was similar (0.82, 95% CI 0.67 to 1.01). There were many fewer studies in the 24-hour group which may have led to this non-significant RR. The HIP ATTACK group recently performed a large randomized controlled study of 69 hospitals in 17 countries evaluating if even more accelerated fixation (defined as within 6 hours of admission) would benefit patients.17 This group compared fixation times of <6 hours with patients undergoing fixation within 24 hours and found that there was no difference in mortality (HR 0.97, 95% CI 0.83 to 1.13) or major complications (HR 0.91, 95% CI 0.72 to 1.14). Although there was no significant benefit, it was also not associated with any increased risk. We chose 24 hours as our “ideal” fixation time based on previous studies, as well as the fact that only 27 (6.8%) patients in our study had femur fixation later than 48 hours, which limited our statistical analysis.
Early repair has been hypothesized to improve outcomes for multiple reasons. Until patients’ fractures are repaired, these patients are on full bed rest and at risk of muscle mass loss and increased deconditioning, which put them at higher risk for falls down the road.18 19 Bed rest also increases patients’ risk of delirium.20 Early mobility after surgery has been associated with significantly decreased delirium rates and decreased lengths of stay in postsurgical elderly patients.21 Increased lengths of hospital stay have been associated with increased risk of nosocomial infections22 23 and increased hospital costs.24 The pain and bleeding from the fracture lead to increased stress state, sympathetic activation, and activation of inflammatory, hypercoagulable, and catabolic states.25–27 Earlier surgery may reduce the time patients spend in these high stress states and may lead to decreased inflammation, improved healing, improved blood pressure control, less risk of myocardial infarction, venous thromboembolism, etc, and may account for decreased complications and mortality.
We did not find any significant patient factors that were associated with delayed fixation, and although our rates of delayed fixation are lower than some previous articles, our aim is to repair all patients with fractures within 24 hours if it can be safely done. The orthopedic service at our trauma center has a designated surgeon covering only orthopedic trauma with a designated operating room every weekday. However, operating room access on weekends is less predictable, as orthopedic cases may be delayed for more “emergent cases” given the limited number of anesthesia staff and nursing available on weekend days. This could be a potential source of delayed fixation and could be improved by increasing staffing of operating rooms on weekend days. Further research should address this question. Patients admitted to the medical service at admission had a higher likelihood of delayed fixation greater than 24 hours after admission. The number of patients admitted to the medicine service was quite low in our study, but still was notable for the significantly higher rate of delayed fixation. Detailed chart review of the patients admitted to the medical service who had delayed fixation found that, although these patients all had complex comorbidities, in only 1 of the 16 patients were any interventions performed to modify their risk for surgery (one patient required dialysis prior to surgery for volume overload). The remainder had no identifiable change or intervention implemented prior to surgery. This finding is echoed in the HIP ATTACK trial’s17 subgroup analysis looking at the risk of mortality or major complications in patients who had an elevated troponin prior to randomization. In this high-risk subgroup, the authors found that accelerated surgery was still favored. Further research is needed to clarify who is best served by further preoperative optimization versus early surgery. However, we think that our findings support the need for patients with surgical problems to be admitted to a surgical service to place the focus and onus on the treatment team to expedite care.
In our study cohort, we elected to include all patients with any femur fractures, as our trauma and orthopedic group has focused on repairing all fractures within 24 hours of admission as our goal. However, to account for the great diversity in femur fractures (distal, comminuted, etc) that are included in our entire cohort, we thought it important to evaluate the more “usual” cohort of older femur fractures to evaluate how transfer time affected this group’s outcomes. Our findings were similar in this group to the overall cohort, and even in analyzing only patients younger than 65, although the risk of complications when surgery was delayed did not quite reach significance, this may be due to the lower number of young patients. We would argue that all patients with femur fractures should have early fixation within 24 hours if at all possible, to expediate care, limit pain, shorten hospital stays, and decrease risk of complications.
Our study was limited by its retrospective nature, which precludes drawing any causal relationships. It is also limited as it was performed at a single institution, which may mean our findings are not generalizable to other rural trauma centers. The time from injury to admission to the initial hospital was also not known, which may have a confounding effect on our results. We did consider using time from initial presentation to time of femur fracture repair; however, as we were not able to directly affect the referring hospital transfer times, we elected to use the time to admission to the trauma center as the “zero” time point for defining femur fixation within 24 hours. We did also perform an analysis using time from admission to the initial hospital (data not shown), with no significant difference in our findings; however, including transfer time in the time to fracture precluded us from evaluating the two separate times (transfer time and time to repair). As we wanted to directly evaluate if transfer time by itself was associated with delays to fixation or patient outcomes, we thought that separating the times out was the correct approach.
Conclusion
Early surgery is not always feasible, and some patients do need optimization prior to fracture fixation, but whenever safe and feasible early fixation should be pursued. We found that repair within 24 hours of admission to our trauma center was associated with a significantly decreased length of stay and decreased complication rate. There was a significantly increased risk of mortality for every hour in femur fracture delay; however, we did not find a significantly increased risk of mortality for patients who had fixation greater than 24 hours after admission. The ideal time to fixation is still unknown. There were no significant relationships between transfer time and time to fixation, complication risk, or mortality; however, our patients were transferred in a reasonable amount of time, without significant delays. Further study to optimize treatment of transferred trauma patients, especially in rural systems, is needed to ensure we are providing the best care possible.
Data availability statement
Data are available upon reasonable request. Data are available as deidentified participant data upon request. Please contact the corresponding author at kristin.colling@essentiahealth.org.
Ethics statements
Acknowledgments
The authors would like to thank and acknowledge Theo Woehrle and Austin Land for assistance with data procurement.
References
Footnotes
Contributors LEL: conception of research question, data acquisition, interpretation of data, drafting of article, final approval. MLH: conception of research question, data acquisition, data analysis, interpretation of data, critical revision of article, final approval. PKK: conception of research question, interpretation of data, critical revision of article, final approval. KPC: conception of research question, data collection, data analysis, data interpretation, drafting of article, critical revision of article, final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on the map(s) in this article does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.