Article Text

Abstract
Background Although the effects of the trauma center(TC) were researched in several studies, there have been few studies on changes in the regional mortality due to the implementation of a TC. An emergency medical center (EMC) and TC were implemented at Nagasaki University Hospital (NUH) for the first time in the Nagasaki medical region of Japan in April 2010 and October 2011, respectively, and they have cooperated with each other in treating trauma patients. The purpose of this study was to investigate the effects on the early mortality at population level of a TC working in cooperation with an EMC.
Methods This is a retrospective study using standardized regional data (ambulance service record) in Nagasaki medical region from April 2007 through March 2017. We included 19,045 trauma patients directly transported from the scene. The outcome measures were prognosis for one week. To examine the association between the implementation of the EMC and TC and mortality at a region, we fit adjusted logistic regression models.
Results The number of patients of each fiscal year increased from 1492 in 2007 to 2101 in 2016. The number of all patients transported to NUH decreased until 2009 to 70, but increased after implementation of the EMC and TC. Overall mortality of all patients in the region improved from 2.3% in 2007 to 1.0% in 2016.In multivariate logistic regression model, odds ratio of death was significantly smaller at 2013 and thereafter if the data from 2007 to 2011 was taken as reference.
Conclusions Implementation of the EMC and TC was associated with early mortality in trauma patients directly transported from the scene by ambulance. Our analysis suggested that the implementation of EMC and TC contributed to the improvement of the early mortality at a regional city with 500000 populations.
Level of evidence Level III.
- trauma center
- population
- mortality
- japan
- emergency medical service
- observational study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Trauma is a major cause of mortality in Japan, especially in young people.1 Some research reports investigated the reduction of mortality at an institution after a quality improvement programme was instituted at a single trauma center (TC).2–4 Several studies have also shown a significant decrease in mortality among severely injured patients treated at hospital with a TC compared with those treated at non-TC hospitals in adults5 and in children.6 7 However, few studies have investigated the changes in regional mortality following the implementation of a TC. An emergency medical center (EMC) and TC were implemented at Nagasaki University Hospital (NUH) for the first time in the Nagasaki medical region of Japan in April 2010 and October 2011, respectively, and they have cooperated with each other in treating trauma patients. We hypothesized that implementation of EMC and TC capable of treating severe trauma patients led to reduction in mortality of 500 000 population medical area. Therefore, the purpose of this study was to investigate the effects on the early mortality at population level of a TC working in cooperation with an EMC.
Materials and methods
Study design and data
We conducted a retrospective study using standardized regional data (ambulance service records) collected in the Nagasaki medical region. Nagasaki ambulance service has three fire departments and each department has satellite service (total 19 services). In Japan, it is determined by law that all ambulance service should record prehospital transports data. The data were collected for all patients taken to hospitals in an ambulance and included prehospital information and both the definitive diagnosis and outcome at 1 week after injury (returned home, hospitalization, discharged, transferred to a higher-level medical institution, transferred to other institution, death in the emergency room (ER), death after hospitalization). All hospitals in the Nagasaki medical region were encouraged to submit their records (participation rate 100%, collection rate 91.6%). Mortality as the primary outcome of this study was a composite of death in the ER and that after hospitalization.
Study setting
The Nagasaki medical region, with an area of about 456 km2 and population of about 500 000 people, is located in the southern part of Nagasaki prefecture in Japan. There were 26 acute care hospitals in the region in April 2010, at which time NUH implemented an EMC as a tertiary emergency medical institution certified by Nagasaki prefecture. NUH had 862 beds. The EMC had eight beds in its intensive care unit and 19 beds in its high-care unit and was served by nine members including a surgeon, neurosurgeon, orthopedist, anesthesiologist, cardiologist, neurologist, neurosurgeon and emergency physician. They had no duty other than taking care of patients in EMC. There were no regulations at the time on the establishment of a TC in Japan. Therefore, we started with three orthopedists and one plastic surgeon, and they cooperated with the EMC staff and could also consult with the doctors of other departments in the hospital, especially when they cared for severely injured patients.
Ambulance services triaged trauma patients by physiological evaluation (consciousness: Japan Coma Scale ≥100; breathing: respiratory rate <10 or ≥30/min, etc; circulation: systolic blood pressure <90 or ≥200 mm Hg, etc), anatomical evaluation (suspected of flail chest, pelvic fracture, etc), and assessment of injury situation (fellow passenger’s death, rollover accident, etc). Although the triage criteria had existed since the time before implementation of EMC, NUH were not fully ready to accept severe trauma patients. NUH announced publicly before opening EMC that it would aggressively accept critically ill patients hard to treat in the other hospitals and also announced again before opening TC.
Study population
Analyses were performed during April 2007–March 2017. Since EMC was implemented in April 2010 and TC was in October 2011, we defined fiscal 2007 to 2011 as pre-EMC&TC period, and fiscal 2012–2016 as post-EMC&TC period.
There were 13 main diagnostic codes used by the treating physicians. Coding of injuries due to external causes was divided into traumatic intracranial hemorrhage, cardiovascular and lung injury, abdominal organ injury, pelvic fracture, proximal femur fracture, other fractures, severe multiple trauma, spinal cord injury, asphyxia, burn, drowning, poisoning, and minor injuries. Trauma patients directly transported from the scene in the Nagasaki medical region were included in the present study.
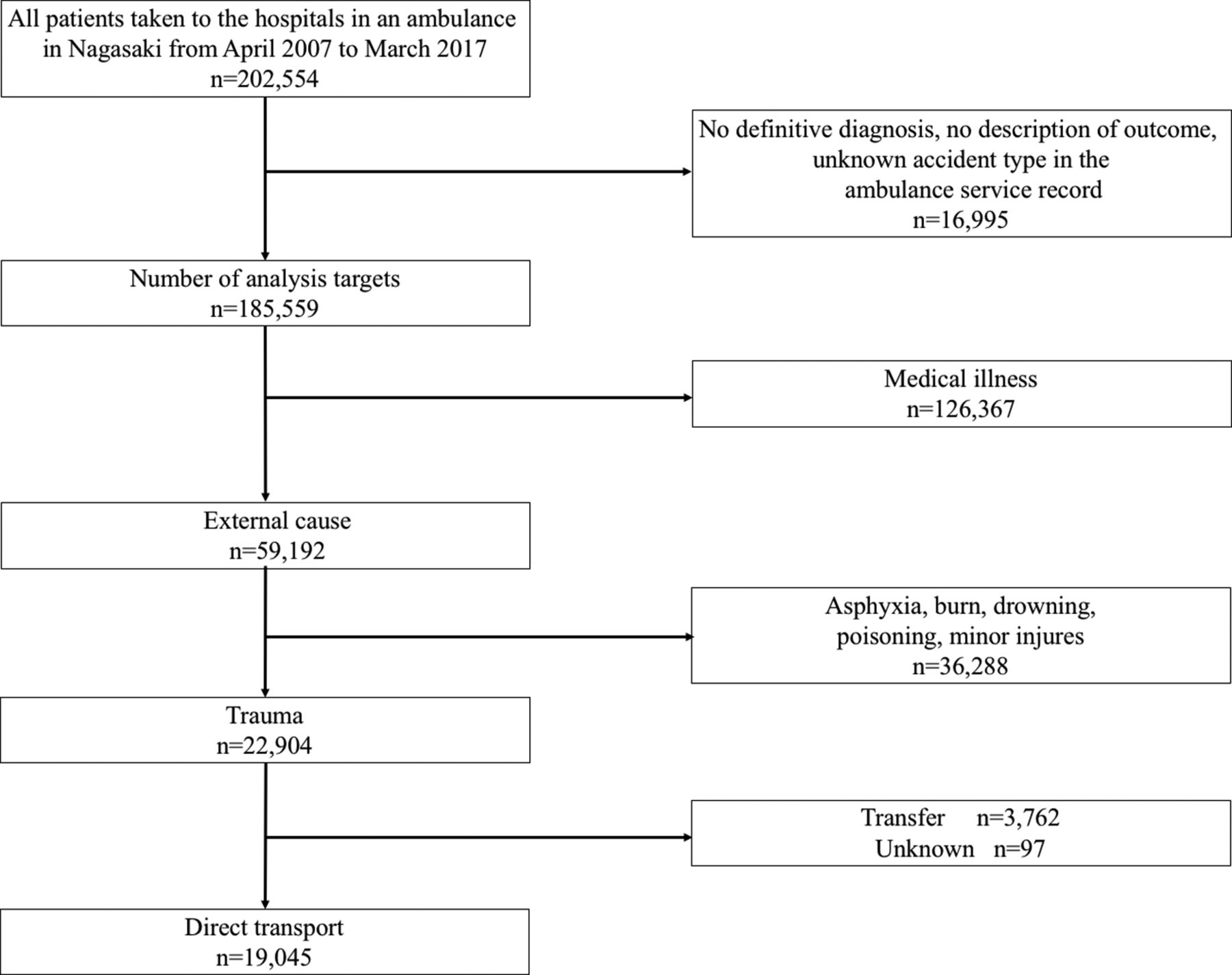
First, we excluded cases with no definitive diagnosis, no description of outcome, and unknown accident type in the ambulance service record (figure 1). Next, cases with medical illness were excluded, and the codes such as asphyxia, burn, drowning, poisoning, and minor injuries including sprains and strains were excluded from cases with an external cause of injury. Thus, trauma patients were defined as those having the following codes: traumatic intracranial hemorrhage, spinal cord injury, cardiovascular and lung injury, abdominal organ injury, pelvic fracture, proximal femur fracture, severe multiple trauma, and other fractures. Finally, we excluded patients transferred from another hospital and those with unknown transport type. Codes selection was performed at the discretion of the treating physicians. Severe multiple trauma was defined as severe injuries involving multiple body regions.

Derivation of the study sample from the standardized regional data in the Nagasaki medical region.
Because of the anonymous nature of the data, the requirement for informed consent was waived.
Statistical analysis
Our analysis investigated the association between mortality and implementation of the EMC and TC. First, we evaluated risk via adjusted OR, 95% CIs, and p values for mortality with multivariable logistic regression models adjusted for years since implementation of the EMC and TC, age, sex, site (NUH vs non-NUH (ie, patients not transported to NUH)), trauma code, and time from emergency call to hospital arrival. We also performed subgroup analyses across three age strata using the above multivariable logistic regression model except for age because ageing of the population was observed throughout the study. In addition, we showed transitions of the number of trauma patients, each injury, age, age subgroup, sex, and time from emergency call every year. Whether these transitions to monotonically increase or decrease were analyzed by a linear regression model. Yearly rates of patients transported to NUH were analyzed by a Poisson regression model. A p value of <0.05 was considered to indicate statistical significance. All analyses were performed using R V.3.5.2 (R Foundation).
Results
From April 2007 to March 2017, 202 554 patients were transported in the region, and the rate of record collection was 91.6% (n=185 559). In total, 19 045 trauma patients directly transported from the scene were eligible for our analyses (figure 1). The number of patients significantly increased each fiscal year from 1492 in 2007 to 2101 in 2016 (online supplemental table). The mean of age significantly increased from 66.7 in 2007 to 72.5 in 2016 (online supplemental table). Both the mean time from emergency call to the scene and that to hospital arrival were significantly increased by 2.4 min and 8.2 min (online supplemental table), respectively, suggesting that the ambulance service was getting worse mainly due to an increase in the number of patient transports. Among the injuries, other fractures occurred most frequently followed by proximal femur fracture, traumatic intracranial hemorrhage, and pelvic fracture, and these four types of injuries significantly increased during the study period (online supplemental table). The number of all patients transported to NUH decreased until 2009 to 70 but tended to increase after implementation of the EMC and TC although rate of transport did not significantly change (online supplemental table). The percentage of patients transported to NUH with cardiovascular and lung injury significantly increased during the study period (online supplemental table). The rate of transportation to NUH for other fractures and proximal femur fracture remained low throughout the study period (online supplemental table). Mortality in non-NUH hospitals increased to 1.9% until 2009 but decreased after 2010 to 0.6% (table 1, figure 2). However, mortality in NUH was high although it tended to decline during the study period. As a result, overall mortality of all patients in the region improved from 2.3% in 2007 to 1.0% in 2016.
Supplemental material
Outcome 1 week after injury

Serial changes in morality. Black line represents overall mortality. *p<0.05 versus mortality of 2007–2011 by multivariable logistic regression model. NUH, transported to Nagasaki University Hospital; non-NUH, transported to non-Nagasaki University Hospital.
The results of the multivariable logistic regression are shown in table 2.
Results of logistic regression model
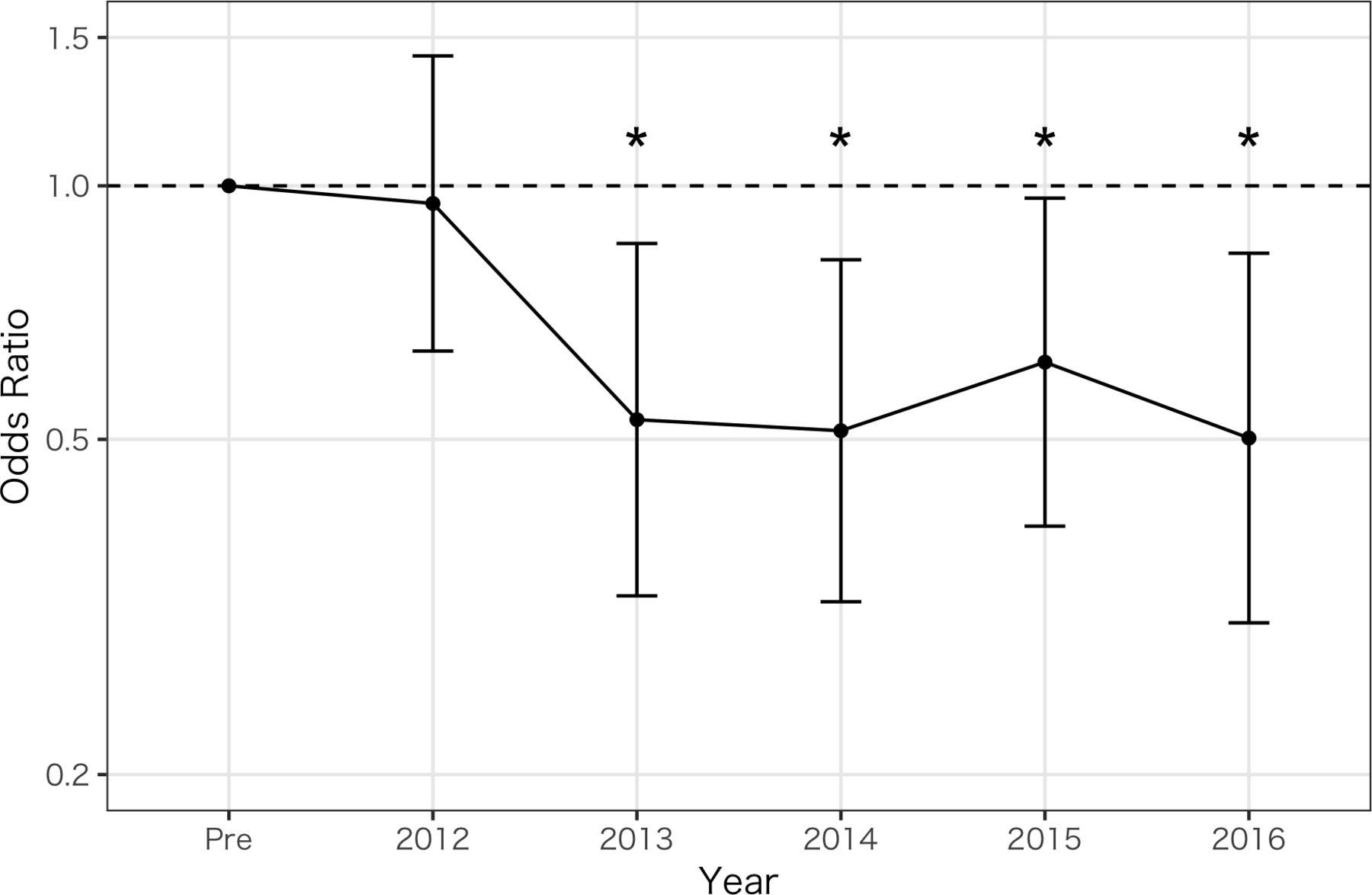
When the data from 2007 to 2011 (pre-EMC&TC period) was used as a reference, ORs of death were significantly smaller in 2013 and thereafter. ORs of traumatic intracranial hemorrhage, cardiovascular and lung injury, abdominal organ injury, pelvic fracture, severe multiple trauma, and spinal cord injury were significantly higher compared with that for proximal femur fracture. OR of transported site (NUH) was significantly high when non-NUH was used as a reference suggesting that more severe patients were transported to NUH. Neither age nor transportation time was significantly associated with mortality. Because ageing of the population was observed throughout the study, we also performed a subgroup analysis of three age groups: pediatrics (0–14 years), adults (15–64 years), and elderly (>64 years). Although only one patient died during the study period, pediatric mortality in the region showed no change. In the adult group, OR of death in 2013 was significantly reduced compared with that from pre-EMC&TC period, and ORs of death in 2015 and 2016 were significantly reduced in the elderly group (tables 1 and 2). These findings indicate that the reduction of mortality in all patients was due not only to the reduction of mortality in the elderly group but also to that in the adult group. Figure 3 shows the ORs of death in each year as a reference with pre-EMC&TC period. During post-EMC&TC period, the ORs were less than 1.0, so the risk of death was low. A significant difference was recognized from fiscal year 2013.

{kind=link}
{kind=link}
{kind=link}
ORs of death in each year as a reference with pre-EMC&TC period. A significant difference is recognized from fiscal year 2013. *p<0.05 versus mortality of 2007–2011 by multivariable logistic regression model.
Discussion
The present study investigated the effects of the implementation of EMC and TC on mortality at a population level. Because the period between implementation of the EMC and TC was short and the two centers cooperated with each other, the single effect of the TC could not be evaluated.
The important feature of this study was that our target was all patients directly transported by ambulance to all hospitals in the region. Previous studies showed that the effects of constructing a trauma system8–12 and the establishment of a trauma center13 14 were particularly efficacious for severe trauma. The number of patients directly transported to NUH increased but the rate of transportation of patients with injuries except for cardiovascular and lung injury did not increase along with implementation of the EMC and TC, probably because the ambulance service triaged the patients appropriately. The decrease in mortality also might result from an increase in the rate of transfer of patients to a higher-level medical institution (table 1). The percentage of transfers to NUH out of those to a higher-level medical institution increased from 6% in 2007 to 31% in 2016 (online supplemental figure). The implementation of the EMC and TC enabled non-NUH hospitals to transfer seriously injured patients promptly to NUH.
Supplemental material
However, mortality in the patients transported to NUH did not show a significant reduction during the study period although it tended to decrease. If EMC and TC receive more trauma patients including those with mild injuries, the mortality rate usually decreases due to the increase in the denominator. The increase in the number of patients transported to NUH was not so large, which suggested that NUH received only seriously injured patients. It may take a longer time to decrease the mortality rate at NUH although a previous study reported that it takes 3 years for a new TC to catch up to a mature TC.14 In the whole region, however, mortality has declined since 2012 after implementation of the EMC and TC, as shown in figure 3, and the decrease reached significance in 2013 (table 2). These findings suggest that the EMC and TC of NUH had beneficial effects on the region.
One report found that mortality worsened by prolonging the prehospital transportation time.15 In our study, however, although the time was extended, it was not associated with mortality. It might take rather more time to find a hospital to receive patients with mild injury and this may be one of reasons why there was no association with mortality.
Limitations
We acknowledge several limitations in this study. First, our study did not use the Injury Severity Score, a tool for evaluating severity because we could not evaluate it in this ambulance service records. Therefore, we could not analyze mortality adjusted by severity. Second, it is the possibility that advances in clinical practice before and after implementation of the EMC and TC contributed to a decrease in mortality rates. Some studies16 comparing neighboring areas where population and climate are similar showed that a TC still had a beneficial effect on the trauma system. Unfortunately, there were no ambulance service records in other areas in Japan similar to that in Nagasaki prefecture, so such verification could not be performed in the present study. Third, coding was based on personal judgement, so the accuracy of coding was not verified. Also, there was a problem in the definition of each trauma. However, the rate of data collection would decrease by judging codes strictly. It is necessary to investigate methods of accurately performing coding without increasing the burden of the physician. Fourth, we set prognosis at 1 week after injury as the measure of outcome. The main causes of death within 1 week are hemorrhagic shock, tension pneumothorax, cardiac tamponade, and brain death, whereas death due to sepsis or multiple organ failure might not be detected. Although most deaths from trauma, occur within 1 week,17 18 long-term critical care of severely injured patients is important and often more difficult, and longer-term outcomes beyond 1 week are relevant to patients. The outcome also did not include the number of deaths after transfer and after 1 week. We need to follow-up longer time outcomes in the future study. Finally, prehospital comorbidity and functional prognosis was not evaluated. We would like to consider revising the ambulance service record in the future.
Conclusion
We performed analyses using ambulance service records to compare early mortality at a population level before and after the implementation of EMC and TC. Although mortality at NUH did not change significantly, mortality at non-NUH hospitals showed a significant reduction after the EMC and TC at NUH was implemented. As a result, a significant improvement in early mortality was observed at a population level. Our analyses suggested that implementation of a single TC working in cooperation with an EMC contributed to the improvement of early mortality in a regional Japanese city with a population of 500 000.
Acknowledgments
We thank Mr Shinji Sugi and Mr Satoru Hayashida for helping with data analysis. We also thank Nagasaki Medical Control Council for permission for use of ambulance service records.
References
Footnotes
Contributors YT, TM and OT conceived the study concept and study design. SS, NM, TM, MO and OT supervised the conduction of the trial and data collection. SS and OT managed the data, including quality control. SS, GT and MO provided statistical advice on study design and analyzed the data. YT drafted the article, and all authors contributed substantially to its revision. YT and OT take responsibility for the paper as a whole, and all authors are in agreement with the content of the article.
Funding This work is supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology in Japan(16H05499, 16K15762).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Study approval was obtained from the institutional review board of Nagasaki University Hospital (approval no.: 18111932).
Provenance and peer review Not commissioned; externally peer reviewed.