Article Text

Abstract
Introduction Rib fractures in elderly patients are associated with increased morbidity and mortality. Predicting which patients are at risk for complications is an area of debate. Current models use anatomic, physiologic or laboratory parameters in isolation to answer this question. The ‘RibScore’ is an anatomic model that assesses fracture severity. Given that frailty is a major driver of adverse outcomes in the elderly, we hypothesize that the combined analysis of fracture severity, physiologic reserve and current pulmonary function are better predictors of respiratory compromise in this population.
Methods This is a retrospective chart review of 263 trauma patients age ≥55 from January 2014 to June 2017. Criteria included blunt mechanism and ≥ 1 rib fracture identified by CT. Variables indicating adverse pulmonary outcomes were defined by: pneumonia, respiratory failure and tracheostomy. Three models were assessed: (1) RibScore, (2) Modified Frailty Index (mFI) and (3) initial partial pressure of carbondioxide (PaCO2).
Results A total of 263 patients met inclusion criteria. 13% developed pulmonary complications. Increased RibScore, mFI and PaCO2 were each statistically associated with risk of complications. Receiver operating characteristics area under the curve analysis of individual models predicted complications with the following concordance statistic (CS): anatomic (RibScore) yielded a CS of 0.79 (95% CI 0.69 to 0.89); physiologic (mFI) yielded a CS of 0.83 (95% CI 0.75 to 0.91) and laboratory (PaCO2) yielded a CS of 0.88 (95% CI 0.80 to 0.95). The PaCO2 had the highest discriminative ability of the three individual models. Combining all three models yielded the best performance with a CS of 0.90 (95% CI 0.81 to 0.97).
Discussion The RibScore maintains discriminative ability in the elderly. However, models based on mFI and PaCO2 individually outperform the RibScore. A combination of all three models yields the highest discriminative ability. This combined approach is best for assessing the severity of rib fractures and prediction of complications in the elderly.
Level of evidence Prognostic Study, Level III.
- rib fractures
- frailty
- elderly
- respiratory failure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Rib fractures occur in nearly 10% of patients with blunt trauma.1 The pain associated with rib fractures leads to poor pulmonary hygiene and associated pneumonia, respiratory failure, empyema, acute respiratory distress syndrome and prolonged hospitalization. These pulmonary complications are more pronounced and are linked to an increased mortality rate in the elderly population.2 In a study by Bulger and colleagues, patients aged 65 years and older with more than four rib fractures were more likely to suffer complications than those younger than 65. Furthermore, when compared with the younger group, the elderly population had higher numbers of ventilator days and intensive care unit (ICU) length of stay as well as higher rates of pneumonia and death.3
Attempts to quantify risk beyond one’s chronological age and towards medical comorbidities and functional decline defines what we have come to know as frailty. Frailty has been shown to be an independent risk factor over age.4 This is a state of vulnerability with reduced physiologic reserve and affects the capacity to maintain or regain homeostasis when exposed to stressors and places patients at increased risk of complications.5 Despite agreement on its definition, there is little agreement on which frailty index is best.6 Many of the existing frailty scores are too exhaustive and not practical for clinical assessment. The Modified Frailty Index (mFI), however, was the first of its kind to be validated in surgical patients by combining variables from the Canadian Study on Health and Ageing Frailty Index with those of the American College of Surgeons National Surgical Quality Improvement Programme (NSQIP).4 The mFI, which represents an accumulation of deficits, is more practical in its use in a busy hospital setting and allows for early identification of patients with limited physiologic reserve. Timely intervention and mobilization of resources is paramount across the continuum of trauma care, and the mFI is an ideal model of frailty in the trauma setting.
Multiple authors have shown that increased number of fractured ribs and the locations of those fractures are risk factors for respiratory compromise and death.3 7–9 Chapman et al was the first to describe a scoring system for rib fractures, called the RibScore, that defined anatomic variables to predict patient outcomes.9 The authors concluded that an increasing RibScore was linearly associated with three complications of interest: pneumonia, acute respiratory failure and the need for tracheostomy. The average age of patients in this study was 48 with a median injury severity score (ISS) of 17. The rate of complications in this relatively young population elicits concern for an osteoporotic elderly population who are likely to incur similar adverse pulmonary events with far less injury severity.
The aim of our study was to assess the utility of the RibScore, the mFI and a baseline partial pressure of carbondioxide (PaCO2) level as clinical assessment tools in the injured geriatric patient with rib fractures. We chose these three models as they have been shown to be useful in risk assessment and at the same time are easily obtained during initial presentation to the emergency room. We hypothesized that in elderly patients, where frailty is a major driver of adverse outcomes, a purely anatomic model would be insufficient for predicting outcomes. We proposed that a combined model that takes into account physiologic reserve (ie, mFI) and current pulmonary status (ie, initial PaCO2) would yield higher discriminative ability.
Methods
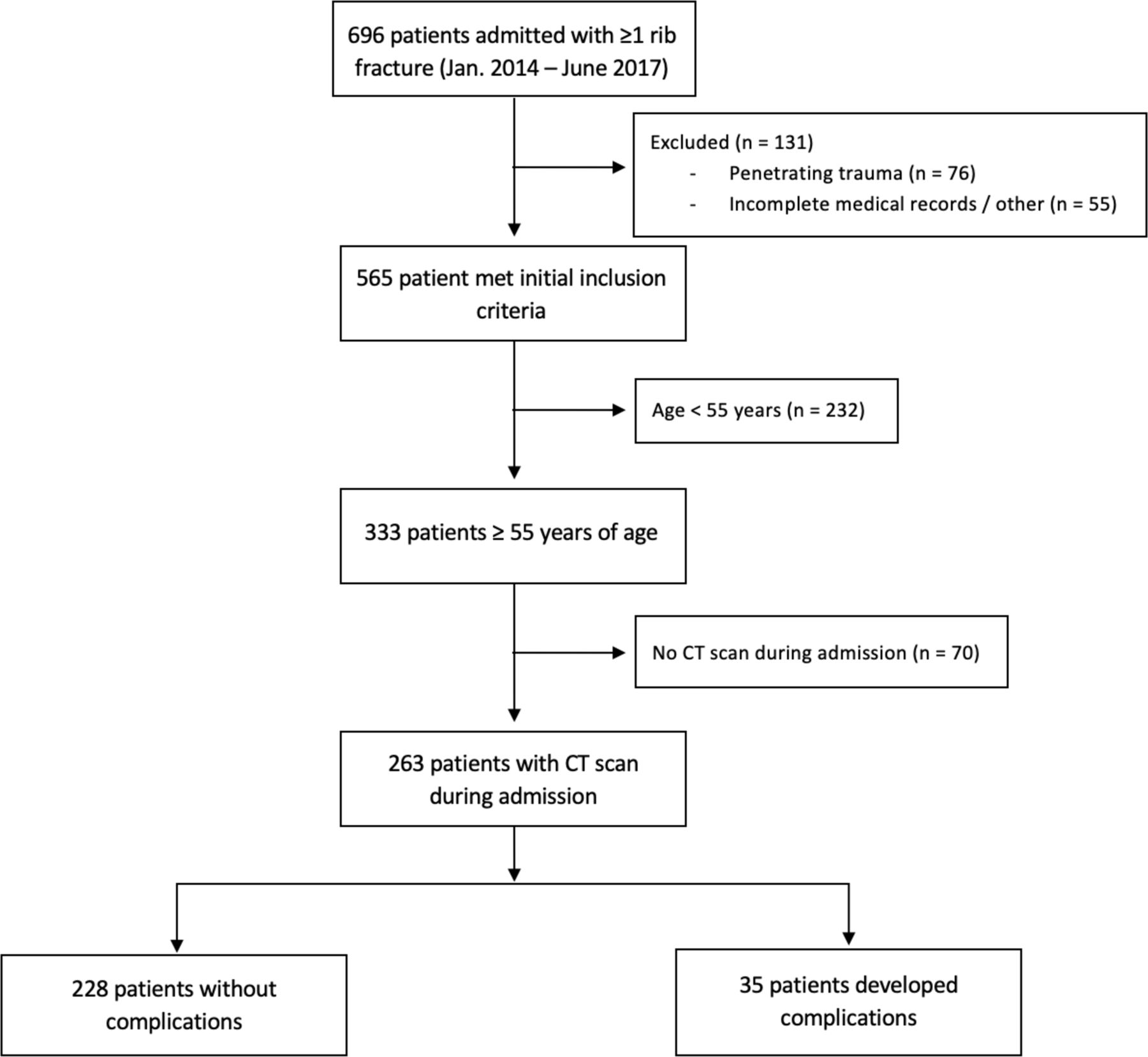
After Institutional Review Board (IRB) approval, we retrospectively reviewed all patients in our center’s level one trauma registry with a diagnosis of one or more rib fractures from January 2014 to June 2017 (figure 1). We excluded patients with penetrating trauma, incomplete medical records, and patients who were pregnant. We further limited our analysis to patients who were 55 years of age or older who underwent a chest CT scan during admission. The age of 55 was chosen based on institutional practice patterns described below.
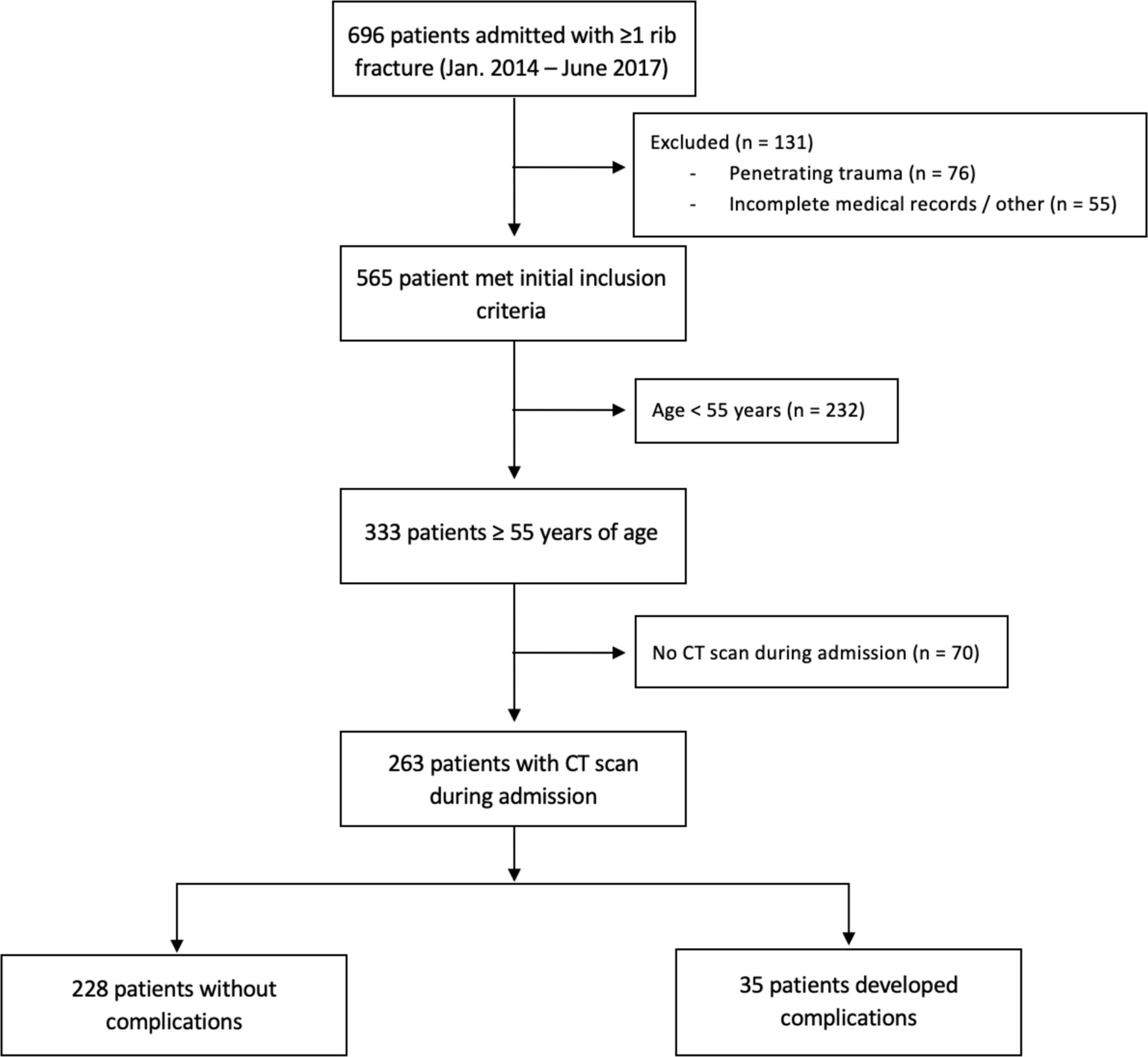
Flow chart of patients meeting inclusion criteria.
The following demographics were extracted from the database: age, gender, ISS, a history of comorbidities, history of smoking and associated injuries. All patients presenting to the emergency department per protocol receive an arterial blood gas within 60 min of presentation. The data from the arterial blood gas was collected for each patient.
Associated injuries were obtained via our institution’s trauma registry. Injuries included the following: head injuries including skull fractures, epidural or subdural hematoma or other intracranial hemorrhage; pulmonary contusions or lacerations; abdominal injuries including solid organ hematomas; hemothorax or pneumothorax identified radiographically and fractures of the clavicle, sternum, scapula, spine, pelvis or facial bones.
The RibScore is an anatomic score that has been proposed as a model to predict the subsequent inpatient course of patients presenting with rib fractures.9 The CT scans of each patient were reviewed to extract the six components of the RibScore which are as follows: (1) ≥6 total rib fractures; (2) severe rib fractures ≥3 (bicortical displacement); (3) presence of flail chest (≥3 consecutive ribs fractured in two or more places); (4) bilateral rib fractures; (5) first rib fracture and (6) at least one fracture in three anatomic locations. The RibScore was subsequently calculated for each patient.
The mFI is a functional score that has been developed as a measure of preoperative morbidity and has been validated in numerous studies as an accurate and useful tool in predicting postoperative morbidity.4 10 The mFI is calculated as a combination of 11 functional preoperative conditions: non-independent functional status; history of either chronic obstructive pulmonary disease or pneumonia; history of diabetes mellitus; hypertension requiring the use of medications; history of congestive heart failure; history of myocardial infarction; history of percutaneous coronary intervention, cardiac surgery or angina; peripheral vascular disease or rest pain; transient ischemic attack or cerebrovascular accident without residual deficit; cerebrovascular accident with deficit and impaired sensorium. The mFI is reported as a score ranging from 0 to 1 and is a fractional value calculated as the number of positive variables in the patient’s medical history divided by the total of 11 possible variables.
Three different models were then developed to assess outcomes: an anatomic model of injury severity based on the RibScore; a model of physiologic reserve based on the mFI and a model of current pulmonary status based on initial PaCO2 within 60 min from presentation to the emergency department.
The primary outcomes were similar to those in the original RibScore article which were the development of pneumonia, respiratory failure and tracheostomy. The development of pneumonia was analyzed clinically based on physician diagnosis. Respiratory failure was defined as mechanical ventilation for ≥48 hours during hospitalization. The need for tracheostomy was at the discretion of the attending physician. Our study assessed the composite risk of developing any one or more of these three complications within 30 days of initial injury. For patients discharged prior to 30 days, outcomes were included in the analysis if they returned to our institution and documentation was present in our system. Any complications that may have occurred at an outside institution within the 30-day window were not included in our analysis.
Statistical analysis
The study population was divided into two subgroups based on the development of complications after the injury (no development of complications vs development of complications). The two groups were examined for differences between their baseline characteristics. Binary variables were compared between the two groups using χ2 or Pearson’s exact test as appropriate. Continuous variables were examined for normality of distribution using the Shapiro-Wilk test. Normally distributed variables were compared between the two groups using Student’s t-test, whereas non-normally distributed variables were compared using the Mann-Whitney U test. Next, a subgroup analysis was performed using only patients aged ≥55 years. The process was replicated as described above. All subsequent analyses were performed in that subgroup of patients (≥55 years old).
The different components of the RibScore were compared between the two groups using the aforementioned tests to assess for differences between the two groups. All baseline differences between the two groups that differed at a p<0.05 were inserted in a logistic regression with the dependent variable being subsequent development of complications. All of the components of the RibScore were inserted in the model to assess the impact of the different anatomic components on the outcome. Adjusted ORs with adjusted p values were derived from the multivariate analysis.
To identify independent predictors of developing complications in the elderly population (aged ≥55 years), a forward stepwise logistic regression was performed, inserting variables that differed at a p<0.2 between the two groups in the univariate analysis. Next, subsequent multivariate analyses were performed with the independent variable being the development of complications. Independent variables were all independent predictors identified from the stepwise forward logistic regression. To assess which of the three models has a higher predictive ability, each model was inserted in the logistic regression in a stepwise fashion. Receiver operating characteristics (ROC) and area under the curve (AUC) classification analysis was used to analyze which of these models can predict the diagnostic ability of a binary classifier model when its discrimination threshold is varied.
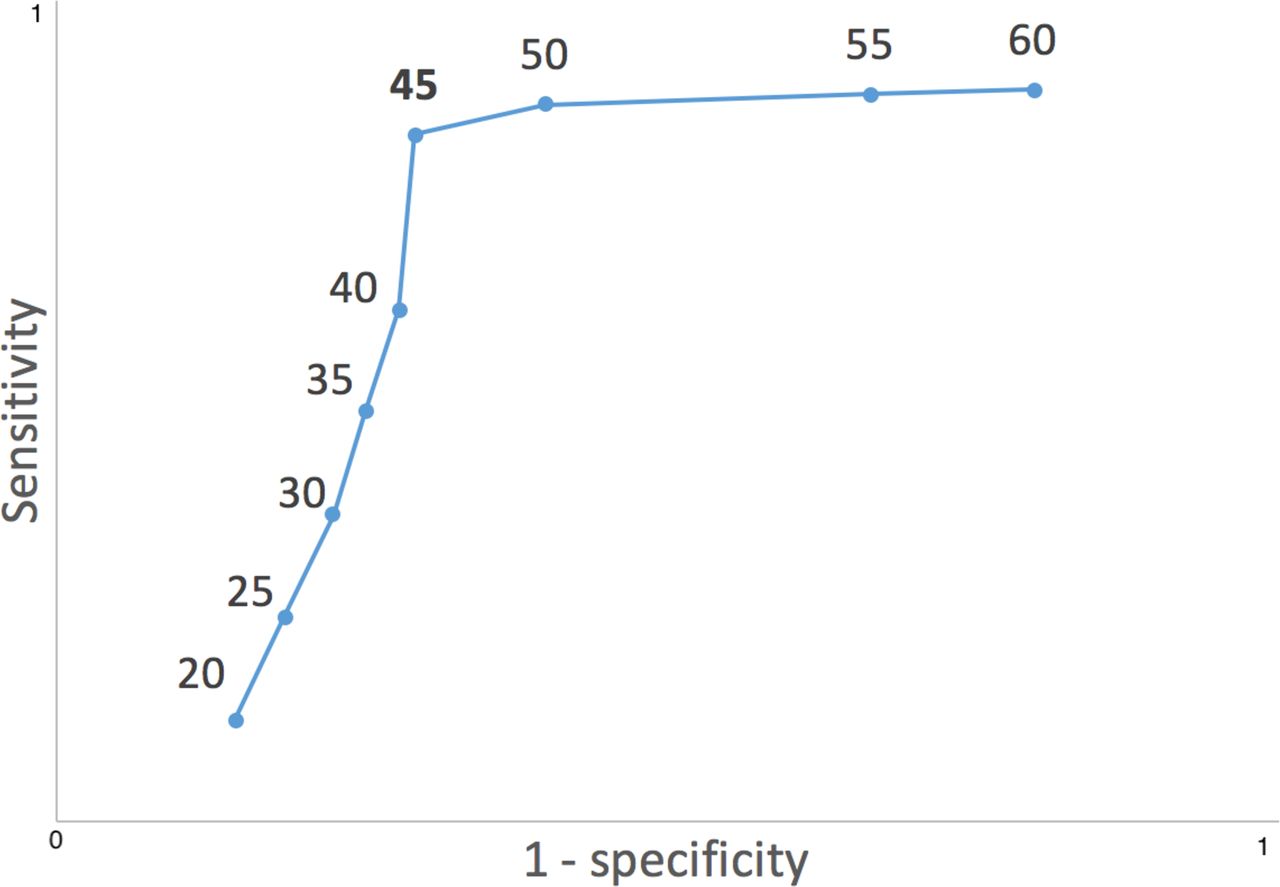
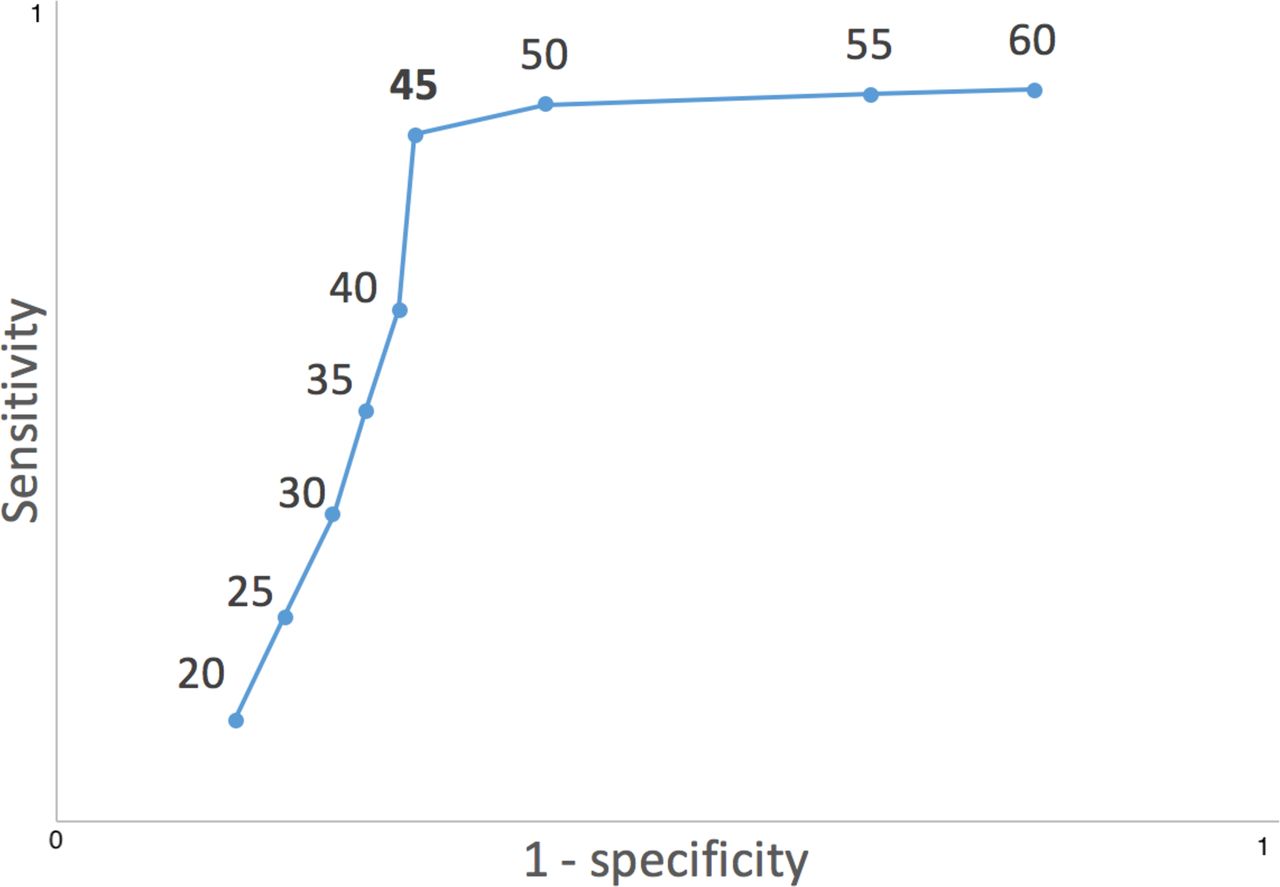
Once the PaCO2 model proved to have the highest predictive ability, a cut-off analysis was deployed. Multiple regression models for development of complications were deployed correcting for differences in univariate analysis at p<0.05 for various PaCO2 cut-off points. The AUC and the R2 were calculated for each model, which was subsequently plotted in an ROC curve. The PaCO2 value used in the regression with the highest AUC was selected as the cut-off that best explained the development of complications. All statistical analyses were performed using the SPSS Windows V.12.0.
Results
During the study period, a total of 263 patients aged ≥55 years were identified and were included in the analyses. A total of 228 patients did not develop any complications, whereas 35 patients did develop complications. The incidence of each complication was as follows: pneumonia only, 10; respiratory failure only, 9; tracheostomy only, 0; pneumonia and respiratory failure only, 9; pneumonia and tracheostomy only, 0; tracheostomy and respiratory failure only, 1; pneumonia, tracheostomy and respiratory failure, 6. A total of six patients included in our analysis died within 30 days of initial injury. Of that group, all six suffered at least one pulmonary complication (ie, respiratory failure, tracheostomy or pneumonia). The figure 1 depicts the study population after exclusion of patients who did not meet our inclusion criteria.
Table 1 depicts the demographics and baseline characteristics of the study population. The mean age of the study population was 63 years (SD 13). For those who developed complications, the mean age was 64 years (SD 15) compared with 62 years (SD 10) for those who did not develop complications. The majority of the patients were male (62%) and were mildly injured (ISS<15, 80%). The most common comorbidity was hypertension (66%), followed by hyperlipidemia (43%) and diabetes (26%). The patients that developed complications were more likely to have an associated head injury (40% vs 14%), facial trauma (23% vs 7%), pulmonary contusions (17% vs 3%), clavicular fractures (14% vs 5%), spinal injuries (43% vs 15%) and pelvic fractures (table 1).
Patients’ demographics and clinical characteristics
The table 2 shows the different individual components of the RibScore and complications in the elderly population. Patients that developed complications were more likely to have more than six rib fractures compared with their counterparts (40% vs 15%, p<0.001), bilateral rib fractures (37% vs 10%, p<0.001) and at least one rib fracture in three anatomic locations (17% vs 6%, p=0.027). Patients with complications had a significantly higher incidence of RibScores of three and above (table 2). When a multivariate analysis was deployed adjusting for demographics and associated injuries, including head injuries, none of the separate components of the RibScore had a significant impact on development of complications (table 3).
Association of RibScore components and development of complications in the elderly population
Multivariate analysis of separate RibScore components and development of complications
The table 4 depicts the variables that independently were associated with development of complications. ISS >25, RibScore, initial PaCO2 at admission, mFI, pelvic fractures and pulmonary contusions were all independently associated with increased risk of complications. The R2 for the model was 0.438. The concordance statistic (CS) for the model was 0.90 (95% CI 0.81 to 0.97) with a p<0.001.
Independent predictors of development of complications
Next, to identify the predictive value of the different scores, separate multivariate analyses were performed. All of those models included all of the independent variables that were found to be associated with an increased risk of developing postoperative complications as depicted in table 4. The three different scores (anatomic—RibScore; physiologic—mFI and laboratory—PaCO2) were added in the models in a stepwise fashion and the CS for each model was calculated. When only the anatomic score was inserted, the CS was the lowest (0.79 (95% CI 0.69 to 0.89)). The use of the initial PaCO2 yielded the highest CS out of all the singular models (when a single individual score was used and not a combination of scores, table 5). When the different scores were combined in models, the combination of anatomic and physiologic scores yielded the lowest CS, whereas the combination of physiologic and PaCO2 scores had the highest predictive ability (table 5). Combining all three scores yielded the highest CS of all the individual models (0.90 (95% CI 0.81 to 0.97), p<0.001). A cut-off analysis for the admission PaCO2 revealed that a cut-off of 45 mm Hg had the highest area under the ROC (95% CI, table 6, figure 2).
Comparing models using anatomic, physiologic and laboratory data to predict development of complications
Cut-off analysis for initial PaCO2 in arterial blood gas
{kind=link}
{kind=link}
Sensitivity and specificity of selected partial pressure of carbondioxide values as cut-off points (units: mm Hg).
Discussion
The management of rib fractures continues to be challenging. Clinical outcomes for this injury are multifactorial and present a real dilemma for prediction models that use independent factors. Management varies across a wide spectrum, and although we have found that many patients do not suffer complications, understanding the morbidity and mortality in those who do suffer complications is necessary for providing preemptive care. A successful model would allow physicians to identify patients most at risk of pulmonary complications and intervene early to reduce adverse outcomes.
A validated method to predict outcomes in this setting would be a powerful tool. The aim of our study was to compare three separate models and their ability to predict outcomes in elderly patients with rib fracture. Blunt chest trauma from falls is unique to elderly patients, and rib fractures are a common sequela of this mechanism. There are physiological, anatomic and pathological features that elderly patients share that differentiate them from younger cohorts. For example, we know that mortality from blunt chest trauma nearly doubles in elderly patients compared with younger ones. Moreover, with each additional rib fracture in an elderly patient, the risk of pneumonia increases by 27% and mortality increases by 19%.3 A validated scoring system, therefore, is of particular interest in this population and was the focus of our study.
The age that defined our elderly population (aged ≥55 years) may not appear to meet the social norm of what most people consider to be elder. Prior literature, however, suggests that even relatively young patients may be at a higher risk of complications from rib fractures. For example, Perdue et al demonstrated that age-related morbidity increased in non-elderly patients.11 Similarly, studies by Holcomb and Easter have demonstrated that patients over the age of 45 and even those as young as 40 exhibit increased mortality from rib fractures, respectively.12 13 Based on the review of a series of published data, guidelines at our institution recommend that patients aged ≥55 years with more than one rib fracture be admitted to an ICU monitored bed. For these reasons, we chose age 55 as the cut-off for our elderly population.
Using patient age as a factor to drive medical decision-making, as described above, is common across healthcare. Chronological age by itself, however, is not necessarily indicative of a patient’s overall state of health. There are many physiological factors that drive patient outcomes, and alternative measures that account for these may lead to more accurate prediction models. Frailty, for example, is a measure to quantify a patient’s physiological age as opposed to their true chronological age.
Our study compared three potential models to predict respiratory complications in patients with rib fracture. These models considered anatomic features of the rib fractures in addition to physiological factors such as frailty and arterial blood gas values. The anatomic model we used, known as the RibScore, has been previously proposed by Chapman et al to predict respiratory complications in patients with rib fracture.9 The mFI and arterial blood gas values are also known to be effective risk assessment tools to predict morbidity and mortality for patients in the surgical and trauma setting.4 10 14
Chapman’s study analyzed the CS individually for pneumonia, respiratory failure and tracheostomy in a younger cohort of patients compared with ours (median age 48 years vs 57 years, respectively). Patient age was shown to positively correlate with risk of complications, but incorporating age into the RibScore resulted in no improvement in its discriminative ability. Their CS was slightly higher in patients with isolated chest wall injuries (0.71 vs 0.77 for pneumonia, 0.72 vs 0.83 for respiratory failure and 0.75 vs 0.87 for tracheostomy). In contrast to Chapman’s study, we analyzed the composite ROC AUC CS for patient’s developing any one or more of these three complications. We found the CS for all patients in our population to be 0.79 for the RibScore. We think that a patient’s physiological age (or frailty), as opposed to their chronological age, is a more sensitive indicator of respiratory complications and that incorporating this into the RibScore would improve its discriminative ability.
Our results showed that mFI is an independent predictor of pulmonary complications in the elderly population and revealed a small, but not negligible, increase in its discriminative ability when compared with the RibScore (CS 0.83 vs 0.79, respectively). This suggests that a model based on frailty may perform at least as equally well as the RibScore. Furthermore, it shows that in addition to the anatomic features that compose the RibScore, frailty is a significant risk factor for predicting pulmonary complications in this patient population.
Initial PaCO2 showed the highest discriminative ability of the three individual models (CS 0.88). A combination of all three models yielded the highest CS of 0.90. This result suggests that initial PaCO2 may serve as a better individual predictor of adverse outcomes than models based on injury severity (ie, RibScore) and frailty. Arterial blood gases are performed routinely in cases of blunt chest trauma, and thus the data is easily obtained in the acute trauma setting.
It is recognized that each of the three models used in our study have their own individual limitations. With these limitations in mind, our goal was to combine models based off anatomic and physiologic variables to increase their predictive value. The RibScore may be limited by several factors, including radiologic interobserver variability. It may also be limited by the selection of patients who undergo a CT scan. For example, severely injured patients who are unstable (presumably with high RibScores) would be unlikely to receive a CT scan during their initial presentation. This may, in part, explain the low number of patients with a RibScore of 5 and 6 in both our present study and Chapman’s study.9 Although the mFI is useful in that its variables are standardized in the NSQIP database, it still relies heavily on thorough and accurate documentation. Of the three models, PaCO2 is the most objective, and this may account for it performing the best of the three individual models.
The three outcomes addressed in our study also have their own limitations. The decision to perform a tracheostomy was based on clinical judgement of the attending physician which may be a source of variability. Our data also does not stratify the timing of intubation, which could obscure pCO2 values for patients who may have been intubated prior to arrival. Additionally, unplanned intubation lasting less than 48 hours, although not defined as respiratory failure in our study, may still represent a significant pulmonary complication.
The scope of our study is also limited by a relatively small population. Although our findings are promising, our results need to be validated with a larger, multicenter study with the data set partitioned into both derivation and validation portions. Our current results can be considered hypothesis generating, and we are currently working on a prospective validation of our findings.
In conclusion, the RibScore maintains discriminative ability in elderly patients with blunt trauma rib fractures. However, models based on mFI and PaCO2 individually outperform the RibScore, and a combination of all three models yields the strongest discriminative ability. Our results suggest that a composite risk assessment tool based on RibScore, initial PaCO2 and mFI can be used to identify patients at risk of respiratory complications. This may serve as a preemptive tool for physicians to intervene early and reduce adverse pulmonary events in elderly patients with rib fracture.
Acknowledgments
The authors would like to extend thanks to the members of the surgery department at Henry Ford Health System whose help and support made this paper possible. During the course of this study, the affiliation of Efstathios Karamanos changed from Henry Ford Health System Department of Surgery to the University of Texas Health San Antonio with the Department of Plastic and Reconstructive Surgery.
References
Footnotes
Contributors NS contributed to the conception and final approval of the article. JB contributed to the data collection. JS and EF contributed to the data analysis. JS, JHP and JLJ critically revised the article. NS, JS and JLJ contributed to the design of the work. NS, JS, EF and JLJ contributed to data interpretation. NS, JB and EF contributed to the drafting and revision of the article.
Competing interests None declared.
Patient consent for publication Not Required
Provenance and peer review Not commissioned; externally peer reviewed.