Article Text

Abstract
Background Opioid administration in postoperative patients has contributed to the opioid crisis by increasing the load of opioids available in the community. Implementation of evidence-based practices is key to optimizing the use of opioids for acute pain control. This study aims to characterize the administration and prescribing practices after emergency laparoscopic general surgery procedures with the goal of identifying areas for improvement.
Methods A retrospective chart review of 200 patients undergoing emergency laparoscopic appendectomies and cholecystectomies was conducted for a 2-year period at a single institution. Eligible patients were opioid-naïve adults admitted through the emergency department. Opioid administration and discharge prescriptions were converted to oral morphine equivalents (OME), and analyzed and compared with published literature and local guidelines.
Results Opioid analgesia was provided as needed to 69% of patients in hospital with average dosing of 26.7 OME/day; comparatively, 99.5% of patients received prescriptions for opioids on discharge at an average dosing of 61.7 OME/day. The average dosing in the discharge prescriptions was not correlated with in-hospital needs (Pearson=−0.04; p=0.56); and higher narcotic doses were associated with combination opioid prescriptions compared with separate opioid prescriptions (73.8 (1.90) vs. 50.1 (1.90) OME/day; p<0.01). This difference was driven by the combination medication, Percocet.
Conclusions In the immediate postoperative period, most patients were managed in hospital with opioid analgesia dosages that fell within guidelines. Nearly all patients were provided with prescriptions for opioids on discharge, these prescriptions both exceeded local guidelines and were not correlated with in-hospital narcotic needs or pain scores.
Level of evidence Level 3 retrospective cohort study.
- opioids
- acute care surgery
- appendectomy
- cholecystectomy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Increasing awareness of the opioid crisis has highlighted the role of surgeons in decreasing opioid exposure after operative procedures. The postsurgical population has been found to be at increased risk for chronic opioid use1 with persistent use rates between 3.0% and 7.7% in the 3 months after surgery.2–4 These estimates do not change significantly between major or minor operations3 and a subpopulation of persistent users escalate their use from low-potency to high-potency narcotics.2
Recent findings indicate that the amount of analgesia generally required for minimally invasive operations is substantially less than what is typically provided,5–7 and only a small subset of the postoperative patient population will have prolonged narcotic requirements.1–3 The unused pills in these prescriptions contribute to a reservoir of narcotics available for misuse and diversion in the community. It is therefore incumbent on the prescribing physician to judiciously prescribe these medications. This is most effectively accomplished by standardizing a treatment approach that is aligned with patient needs. A maximum daily oral dose of 50 mg of morphine has been recommended for opioid-naïve patients with acute pain.8–11 Although studies and guidelines have made recommendations for the elective general surgery setting, no such recommendations currently exist in the emergency surgery setting.12 13
Given the recent surge in best practice literature in this area, we undertook to evaluate the in-hospital administration and discharge prescription practices for narcotic analgesia at our institution for patients undergoing minimally invasive emergency general surgery. Our aim was to compare our findings to current guidelines and identify areas for optimizing and standardizing pain management practices for this population.
Methods
Study design
This study was a retrospective chart review examining in-hospital administration and discharge prescribing practices of opioid and non-opioid analgesia after minimally invasive emergency laparoscopic surgery. The goal was to gauge patient needs from in-hospital consumption and determine if this correlated with the discharge prescription. Subsequently, we developed standardized prescribing guidelines based on these findings as well as a literature review.
Subjects
We included adult (aged ≥18 years) patients presenting to the emergency department between October 2015 and September 2017 with diagnoses of either acute biliary tract stone disease (acute crescendo biliary colic, acute cholecystitis) or acute appendicitis and who underwent laparoscopic cholecystectomy or laparoscopic appendectomy, respectively. These patients were all admitted to the emergency general surgical service and had their pain managed exclusively by the surgical team. Patients were excluded if they were admitted from another care facility, were not opioid naïve at the time of admission (defined as a current prescription of ≥60 oral morphine equivalents (OME) per day for ≥7 days), or had a history of opioid use disorder. Patients were also excluded if they underwent a second procedure during the index admission, such as endoscopic retrograde cholangiopancreatography for gallstone pancreatitis, had conversion to an open procedure, if they had an extended length of stay (LOS; ≥5 days), were pregnant, had their pain managed by the pain service rather than the surgical team, or had incomplete records. Our aim was to identify a homogeneous cohort of patients such that pain management could be standardized. To adequately power our study, we sought to review 100 charts for each procedure (see sample size estimates below). As there were more subjects meeting inclusion criteria than required, we randomly subsampled the available patients. Ultimately, the findings related to both appendectomy and cholecystectomy were similar and the results were pooled.
Outcomes of interest
The outcomes of interest were quantity and timing of administration of narcotic and non-narcotic analgesia provided postoperatively on the ward, the associated pain scores while in hospital, and the type and dosing of analgesia provided in the discharge prescription. All opioid doses were converted to OME to facilitate comparisons. Patients were categorized into one of four patterns based on their needs while in hospital: (1) opioid and non-opioid analgesia—defined as those who received both opioid and non-opioid analgesia, this included combination opioids, consisting of a single tablet containing both opioid and non-opioid medication, specifically Percocet (acetaminophen 325 mg/oxycodone 5 mg); (2) opioid-only analgesia, defined as those who received only opioids while in hospital; (3) non-opioid analgesia only; (4) no analgesia at all.
In regard to standard practices at the time of study, there was no standardized pain management guideline or pathway in hospital or for discharge prescriptions. Pain management was determined by a physician assistant and surgical residents. They were supervised by 12 faculty attendings. Patients did not routinely receive intraoperative nerve blocks, nor intravenous Toradol or acetaminophen. There are no electronic health order sets or prescription templates for prescribing. Prescribed opioids included hydromorphone, morphine, Percocet, oxycodone, and Tylenol #3.
Patient demographic information (age, gender, diagnosis, history of opioid abuse and comorbidities) was recorded for all eligible patients, as was the postoperative LOS from arrival on the surgical ward to discharge from hospital in hours, the timing of analgesic medication administration, the last documented numerical pain score (scale of 1–10) within 12 hours of discharge, and the discharge prescription. The discharge prescription daily dosing was calculated as the maximum as-needed dosing available as specified in the prescription.
Because the average LOS on the postoperative ward was less than 24 hours, opioid dosing was calculated hourly according to the formula: Hourly dosing=(total dose)/(hours on ward). To facilitate comparisons this value was then extrapolated to the 24 hours’ dosing.
Statistical analysis
Based on the findings of Hill et al13 we assumed an SD of 85 mg OMEs in the discharge prescriptions. Combined with an error tolerance of 17 mg OME (10% of the mean) and the assumption of normality (Z=1.96), we estimated requiring a sample size of ≥90 for each category. Therefore, we collected two bins of n=100, corresponding to cholecystectomies and appendectomies (total n=200). Differences in dosing and pain scores were calculated with two-tailed t-tests, whereas significant correlations were calculated using t-tests of Pearson correlations. Reported values are means and their associated SEM. Significance was established at p≤0.05, analysis was completed in Excel 2010.
Results
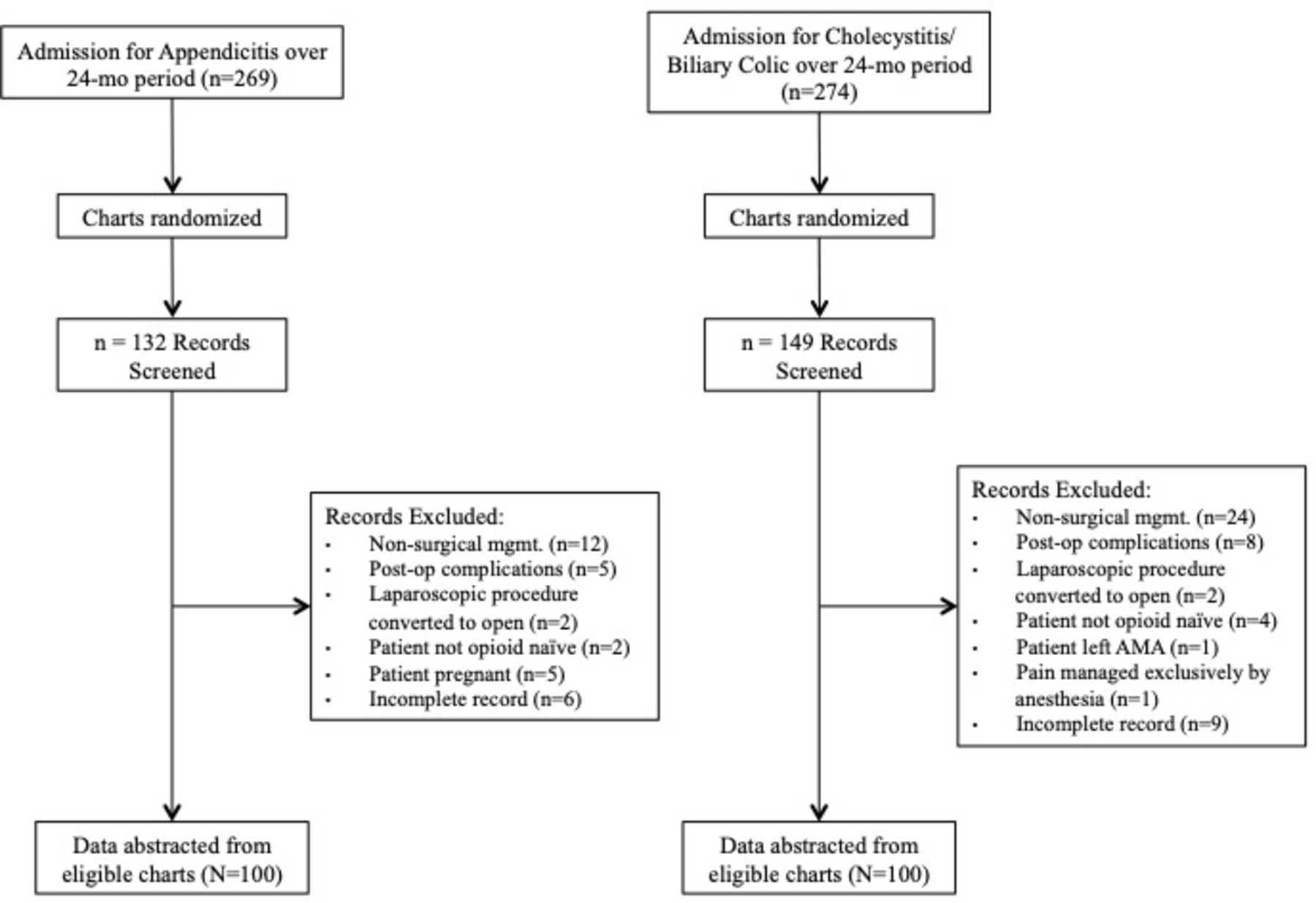
In the 24 months’ period that was examined, a total of 543 patients were admitted to the emergency department for either acute appendicitis (n=269) or cholecystitis/crescendo biliary colic (n=274). These charts were randomly subsampled and screened until data had been abstracted from 100 appendectomy and 100 cholecystectomy charts (figure 1). As there was no significant difference between the hourly opioid dosing on the ward for appendectomies and cholecystectomies (p=0.65), nor significant difference in the last documented pain scores (p=0.83), or size of the discharge prescriptions (p=0.74), the results for the two procedures were pooled. Ninety-two (46%) patients were male with a mean age of 47.2 (1.2) years. The mean postoperative LOS on the ward was 20.1 (1.3) hours, with 79% of patients being discharged within 24 hours and 95% discharged within 54 hours.

Consolidated Standards of Reporting Trials (CONSORT) flow diagram. Eligible charts were randomized and screened until the target of n=100 for each of the two groups was met.
Management in hospital
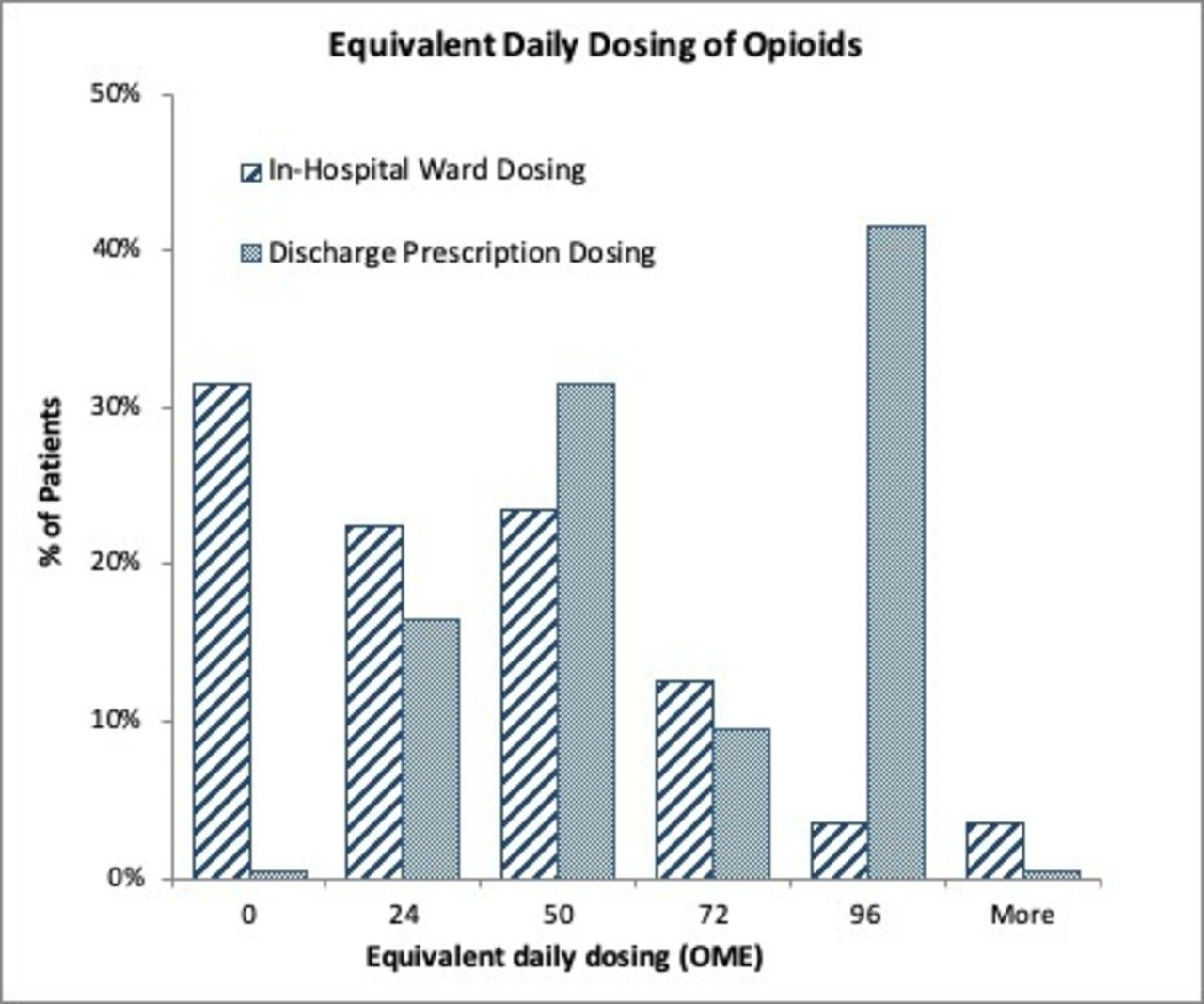
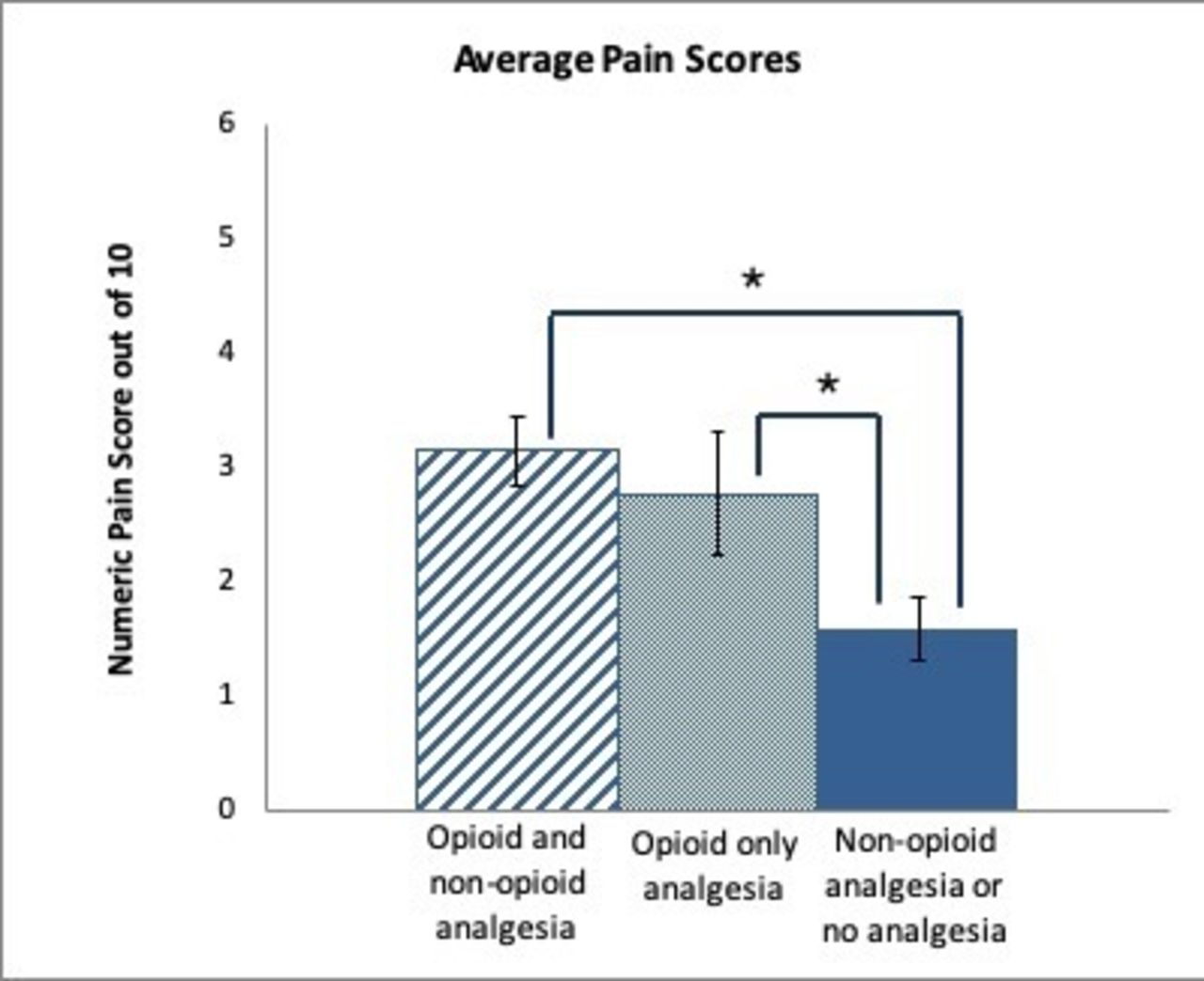
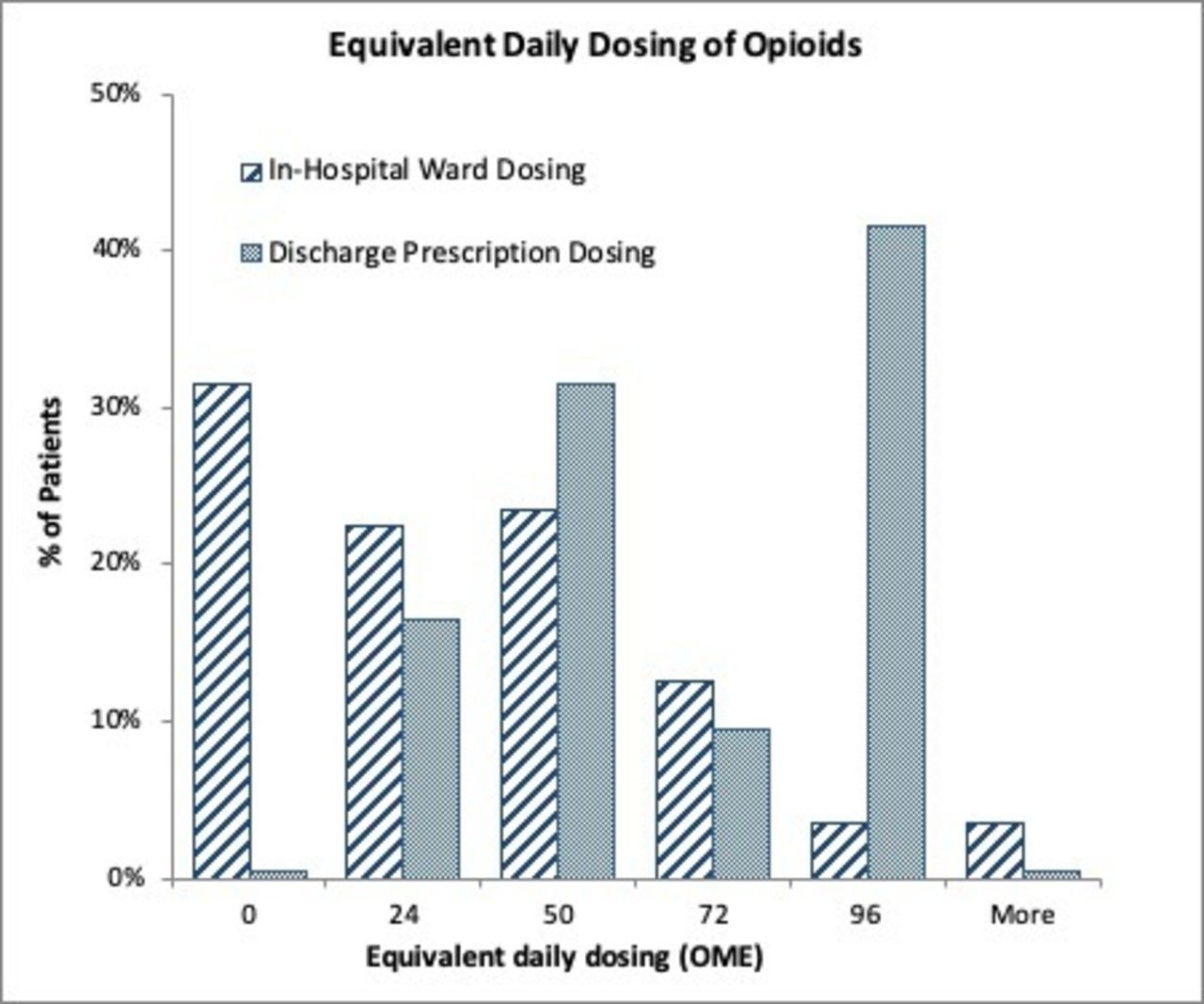
Postoperative patients managed with opioid and non-opioid analgesia in hospital constitute 51% of the cohort, whereas 18% were managed with only opioid analgesia. The remaining 31% used either only non-opioid analgesia (11.5%) or declined any analgesia at all (19.5%) (table 1). The equivalent daily dosing for all patients was 26.7 (2.22) OME. When comparing patients treated with opioid and non-opioid analgesia to opioid-only analgesia, neither the equivalent daily dosing (39.7 (2.17) OME vs. 36.1 (2.21) OME; p=0.65) (figure 2) nor the pain scores (3.5 (0.23) vs. 3.7 (0.23); p=0.83) were significantly different (figure 3). Of all patients, 20.1% required opioid analgesia dosing equivalent of ≥50 OME/day. When non-opioid analgesia was given it was acetaminophen (92.7%), non-steroidal anti-inflammatory drugs (NSAID; 0.8%), or a combination of the two (6.5%).
Postoperative analgesia requirements of emergency general surgery patients in hospital
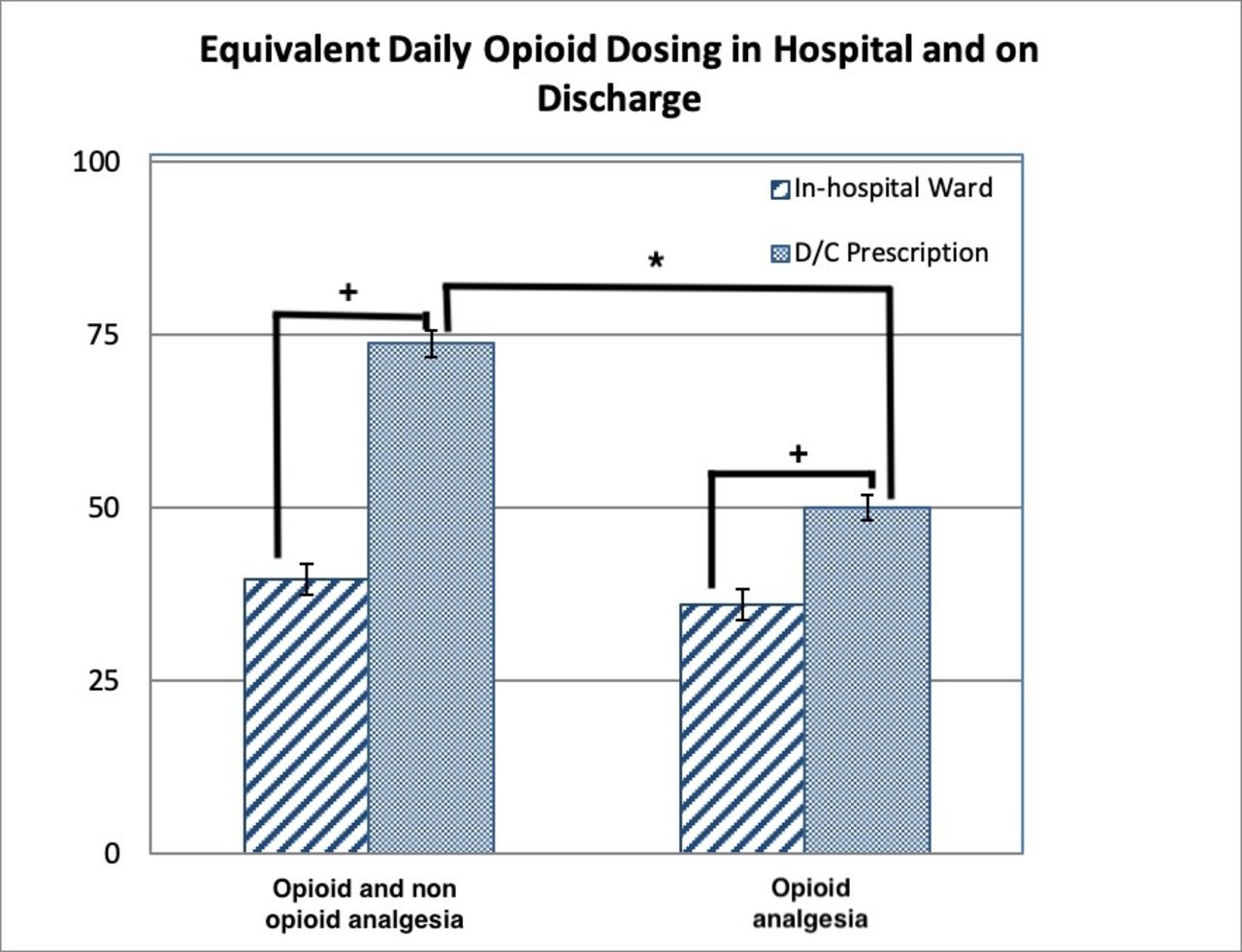
In-hospital compared with discharge (D/C) prescription opioids in oral morphine equivalents (OME) by opioid and non-opioid compared with opioid-only pain management strategies. *Statistically significant with p<0.05. +No correlation.
In-hospital compared with discharge prescription opioids in oral morphine equivalents (OME) per day.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
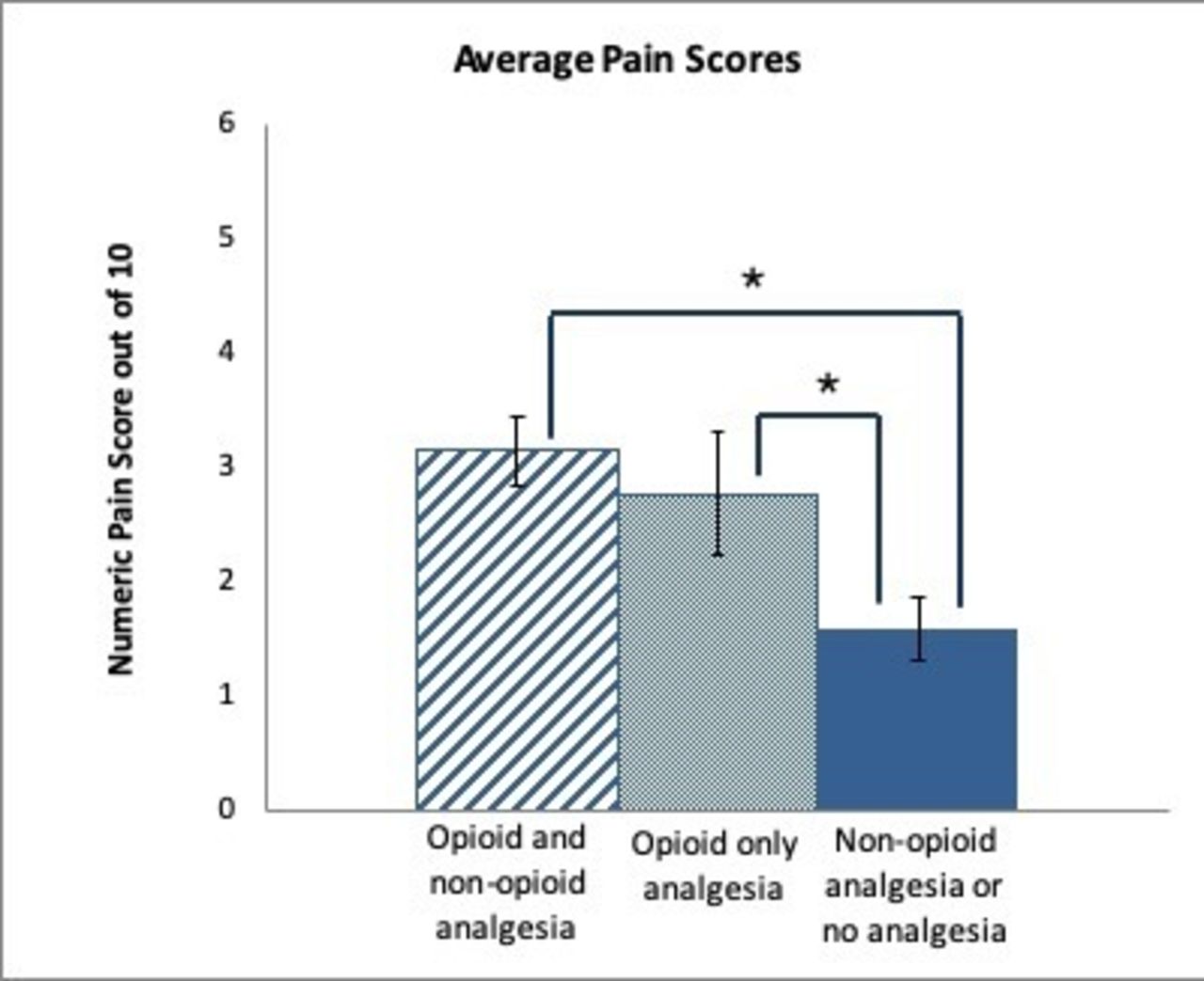
Average numerical pain scores out of 10 recorded within 12 hours prior to discharge. *Statistically significant with p<0.05.
For patients who were managed with opioids and non-opioids in hospital, we examined the time to first administration of the opioid as compared with the non-opioid medication. The average time to the first dose of opioid in patients with a single pill combining an opioid and non-opioid was 4.80 (0.47) hours, as compared with 7.08 (0.58) hours for non-opioid analgesia (table 2). When compared with patients who were managed with separate pills for opioids and non-opioids, the time to first administration was not significantly different (p=0.40).
Average time to first dose of analgesia in hospital for opioid and non-opioid analgesia
Patients managed with opioid and non-opioid analgesia did not report significantly different pain scores from those who were managed with opioids alone (p=0.28). Those who did not use opioids in hospital—which included those who used only non-opioid analgesia or no analgesia at all—reported significantly lower pain scores (p<0.01). Pain scores are shown in figure 3.
Discharge prescriptions
Almost all discharge prescriptions (95.5%) included opioids. Daily dosing was calculated as the maximum as-needed dosing allowable and was equivalent to 61.7 (1.90) OME/day or over twice the opioid dosing made available as an inpatient. At this maximum as-needed dosing, the duration of the prescriptions was found to be 2.6 (0.10) days. On the whole, the average total opioid load of the discharge prescriptions was 143.1 (4.87) OME. The prescription dosing was not correlated with either ward dosing (Pearson=−0.04, p=0.56) or pain score (Pearson=−0.06, p=0.38). Patients who received no opioids on the ward did not receive significantly different prescriptions from those who did (p=0.85). A comparison of in-hospital to discharge OME is shown in figures 2 and 4.
Of all the prescriptions, 49% included opioids and non-opioids. The mean opioid dosing was significantly greater when opioids and non-opioids were prescribed than when opioids only were prescribed (73.8 (1.90) vs. 50.1 (1.90) OME/day; p<0.01). This difference was driven by prescriptions for Percocet—a combined medication of 5 mg oxycodone/325 mg acetaminophen that made up 83% of prescriptions containing both opioids and non-opioids—with a mean opioid dosing of 80.0 (1.20) OME/day. Comparatively, the remaining prescriptions containing opioids and non-opioids, which are composed of two separate medications for an opioid and non-opioid analgesic, had a significantly (p<0.01) lower mean dose of 44.0 (1.30) OME/day. The difference in these doses was not associated with a difference between the in-hospital pain scores for these two subgroups (3.04 (0.21) vs. 3.95 (0.23); p=0.31).
Discussion
This study examined opioid analgesia administration after laparoscopic emergency surgery at a tertiary care academic health sciences center. We chose to focus on this population because pain management should be straightforward in this high-volume patient population that has little risk of prior substance use, a low complication rate, and is unlikely to experience chronic pain. In addition, although guidelines exist for elective prescribing of opioids, none exists to guide prescribing practices after emergency surgery. Eid et al have found the mean number of opioid pills prescribed after emergency laparoscopic appendectomy and cholecystectomy to be 17 (range 0–56) and 17 (range 0–75), respectively.11 However, they did not make recommendations for optimal prescribing practices. Others have made recommendations for discharge prescriptions after elective laparoscopic cholecystectomy of 10–15 opioid pills.13 14 However, there are no studies standardizing prescriptions after common laparoscopic emergency general surgery procedures to our knowledge. Our objective of the current study was to identify discrepancies between current practices and evidence-based guidelines and propose standardized opioid-prescribing practices for laparoscopic emergency general surgery procedures that would not compromise pain control.
This was approached in several ways. First, the amount of opioid and non-opioid analgesia used in hospital was measured and used as a metric for postoperative analgesia requirements. The time to the first administration of analgesia was compared between opioid and non-opioid analgesia to gauge whether opioid analgesia was being used effectively. And finally, the quantity and dosing characteristics of the discharge prescription were compared with in-hospital administration.
We found that the average equivalent daily dose requirement in hospital for postoperative opioid analgesia was 26.7 OME. Eighty percent of these patients required opioid dosing ≤50 OME/day. These results indicate that discharge prescriptions can be reduced to the recommended daily max of 50 OME15 while still meeting the requirements of at least 80% of patients. This target is also in line with the findings of Hill et al13 who found that a standardized prescription meeting the needs of 80% of patients was not associated with increased rates of refill.
Nearly a third of patients (31%) required no opioids on the ward and within this group were 39 patients (19.5%) who required no analgesia at all. This result was consistent with previous findings regarding postoperative opioid requirements after elective laparoscopic cholecystectomies. Chen et al16 found that 35.7% of patients do not require opioids in the first 24 hours after surgery and Hill et al13 found that 34% of patients do no use any of their prescribed opioids after discharge.
When comparing patients treated with opioid analgesia only and those treated with both opioid and non-opioid analgesia, we did not observe an opioid-sparing effect with the addition of non-opioid analgesia as others have found,17 18 as neither the opioid dosing nor pain scores were significantly different between the two groups. That is to say, patients who were given non-opioid analgesia in addition to opioid analgesia consumed the same amount of opioids as those who were given opioids alone. There are three likely explanations for this; first, the opioid-sparing effect is weakest for acetaminophen alone and highest for NSAIDs and cyclooxygenase-2 (COX-2) inhibitors19 and in our cohort, acetaminophen alone was used in 92.7% of patients treated with non-narcotic analgesia. Second, at our institution, patients undergoing minimally invasive operations requiring only short postoperative stays are provided analgesia on an as-needed basis. Comparatively, opioid sparing has been reported when the non-opioid medication is administered at standing doses.18 20 Lastly, the patients who were managed with multimodal analgesia were not being managed by any protocol designed to minimize their opioid consumption. Patients failing opioid-only treatment may be provided with non-opioid analgesia after the initial opioid to augment their pain control. This may explain the shorter time to first administration of opioid analgesics compared with non-opioid analgesics. However, this granular degree of data is not available and may simply reflect common nursing practices.
We found that 62.5% of patients were being treated with non-opioid analgesia while in hospital—a combination of those treated with non-opioid analgesics alone (11.5%) and those treated with both opioids and non-opioids (51%). Research into enhanced recovery after surgery pathways supports the implementation of structured non-opioid analgesia administration schedule postoperatively to reduce postoperative pain and opioid-related side effects.17 In our population, NSAIDs were used very sparingly, likely due to reports of associated complications such as increased risk of bleeding, renal dysfunction, gastrointestinal ulceration, and anastomotic leak. However, there is consistent evidence that NSAIDs are not associated with renal dysfunction in otherwise healthy adults.17 18 Concerns regarding the increased risk of bleeding associated with the COX-1 component of non-selective NSAIDs can be avoided by using COX-2 inhibitors such as Celecoxib.17 19 20 Similarly, anastomotic leak is most pronounced with non-selective NSAIDs and much less so with COX-2 inhibitors (OR=2.13 vs. 1.1621). Haddad et al22 did not observe any increased incidence of anastomotic leaks in emergency general surgery for small-bowel resection/anastomosis.22 Finally, in the context of the laparoscopic cholecystectomies and appendectomies, the risk of this complication is very low, and NSAIDs are likely safe in these patients.
Evaluation of discharge prescriptions revealed three interesting inconsistencies. First, non-opioid analgesia was underused and only included in 49% of discharge prescriptions. However, common non-opioid medications, such as NSAIDs and acetaminophen, are available over the counter and may have been recommended but not recorded in a prescription. Second, the daily maximum dose was significantly different between opioid and non-opioid as compared with opioid-only prescriptions with combination prescriptions being associated with significantly greater opioid exposure. This higher dosing was almost entirely driven by a high number of prescriptions for the combined medication Percocet (5 mg oxycodone/325 mg acetaminophen), which made up 80% of multimodal prescriptions. This significant differential did not correlate with patient needs, as there was no significant difference in the pain scores on the ward for these patients. These data suggest that this combination analgesic, although popular, is not an optimal choice for these patients as it leads to greater opioid availability while potentially limiting the use of non-opioid analgesics (eg, acetaminophen) given the fixed dosing inherent in Percocet tablets. Further, combined medications put patients at risk of surpassing the 4 g/day max of acetaminophen if they unknowingly combine this medication with another acetaminophen medication. Third, the discharge prescriptions did not correlate with patient needs as nearly all included opioids—indicating that discharge prescriptions include opioids by default. Patients who required no opioids in hospital were not given significantly different prescriptions from those who did—a discrepancy that has been previously observed and termed ‘opioid over-prescription’.16 The average daily maximum dose of opioids in the discharge prescription was 61.7 (1.90) OME, with 52% of patients being given prescriptions that were greater than the recommended daily dosing of 50 OME.15 This dosing was on average 2.24 times that which was required on the ward, indicating that the dosing schedule of the prescription is greater than what is likely required. The average duration of prescriptions at the maximum daily dosing was found to be 2.6 (0.10) days, which is less than ≤3 days’ recommendation.15 Taken together, our average prescription size was 143 (4.9) OME total, which is in line with the recommendation of 150 OME during 3 days, but it remains above patients’ documented in-hospital needs.
Our findings are consistent with previous studies that have shown a significant amount of variability in prescribing practices that is independent of patient need and is provider dependent.5 6 11 12 23 24 Providers, concerned about inadequate pain control on discharge, appear to err on the side of overprescribing,25 yet there is little correlation between the rate of refill requests and the size of the discharge prescription5 26 and many prescribed opioids remain unused.7 Further, analgesia duration requirements are generally low with refill rates of 0.4%,13 4.3%12 and 6.8%.26 These trends are concerning because unused prescription medications may be stolen, diverted, or otherwise misused once in the community. Strategies outlined in prior studies suggest that these practices are modifiable without negatively impacting pain scores or rate of refill requests. Specifically, Howard et al reduced discharge prescriptions by 67% without changes in patient pain scores or rates of refill requests27 and Hill et al reduced their prescriptions by 45% while still meeting the analgesia needs of over 80% of discharged patients.13 This more conservative approach is also supported by work into multimodal pain management strategies18 and recent findings that non-opioid analgesia can be as effective as opioid analgesia for managing chronic pain.28 Taken together, our results are consistent with a growing body of evidence that supports standardizing prescribing practices of postoperative opioids.
Limitations
There were a few limitations to this study. First, these data are from a single institution and might simply reflect local practice as evidenced by the significant preference for Percocet as a commonly prescribed analgesic. Second, we made the assumption that the in-hospital as-needed dosing of analgesia was a proxy measure of analgesia requirements after discharge. It is plausible that additional analgesia might be required after discharge when patients are increasingly ambulatory.
In spite of these limitations, there is clear discordance between current practice and guidelines. Based on these findings and expert recommendations, we think the optimal strategy for postoperative analgesia would involve first a separate prescription for standing non-opioid analgesia—including acetaminophen 1000 mg orally every 6 hours ×3 days and ibuprofen 400 mg orally three times a day with meals ×3 days (unless otherwise contraindicated). Second, a prescription for an opioid analgesia with dosing of 50 OME/day. Our institution will be instituting hydromorphone 1 mg orally every 6 hours as needed ×10 tabs. This conservative prescription size is also in agreement with previously proposed guidelines.13 27 For patients who required no opioids in the 24 hours prior to discharge, at the discretion of the provider, this prescription could be eliminated. Third, a structured approach to counseling patients on pain expectations on discharge. Hill et al13 found that 85% of patients who were advised to use NSAIDs or acetaminophen as part of their postop analgesia did so, demonstrating the importance of patient education. Setting expectations is critical as patients should expect to experience some pain, and the aim of analgesia is to decrease their pain enough to mobilize and resume functionality. Patients should be counseled to use opioids for breakthrough pain as opposed to the key component of their pain management strategy. Finally, patients should be advised of options for safe disposal of their unused medication including return to their pharmacy.29 A prospective study is planned based on these results to further evaluate our proposed prescribing strategy.
Acknowledgments
Support was provided by the Sunnybrook Surgical Performance Improvement group working with the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP). Special thanks to Mahsa Sadeghi for support with data collection.
References
Footnotes
Contributors CN: study design, data collection, data analysis, data interpretation, literature review, writing. AN: data interpretation, literature search, critical revision. ABN: study design, data interpretation, literature search, critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This work was approved by the Sunnybrook Health Sciences Centre Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.